Dental Patient Registration Form
Dental Patient Registration Form - I acknowledge that my questions have been answered to my satisfaction. Date relationship to patient 1 patient information 2 dental insurance. I agree that i am responsible for all services rendered to the patient and that payment is. Web take a little time now to save a lot later. Contact your local western dental with any questions! Web dental registration and history. The form is available in a digital, downloadable version or in print. To get started, all new patients need to fill out a new patient registration form. Payment arrangement form name of patient: Web download new dental patient forms to bring to your first dental appointment.
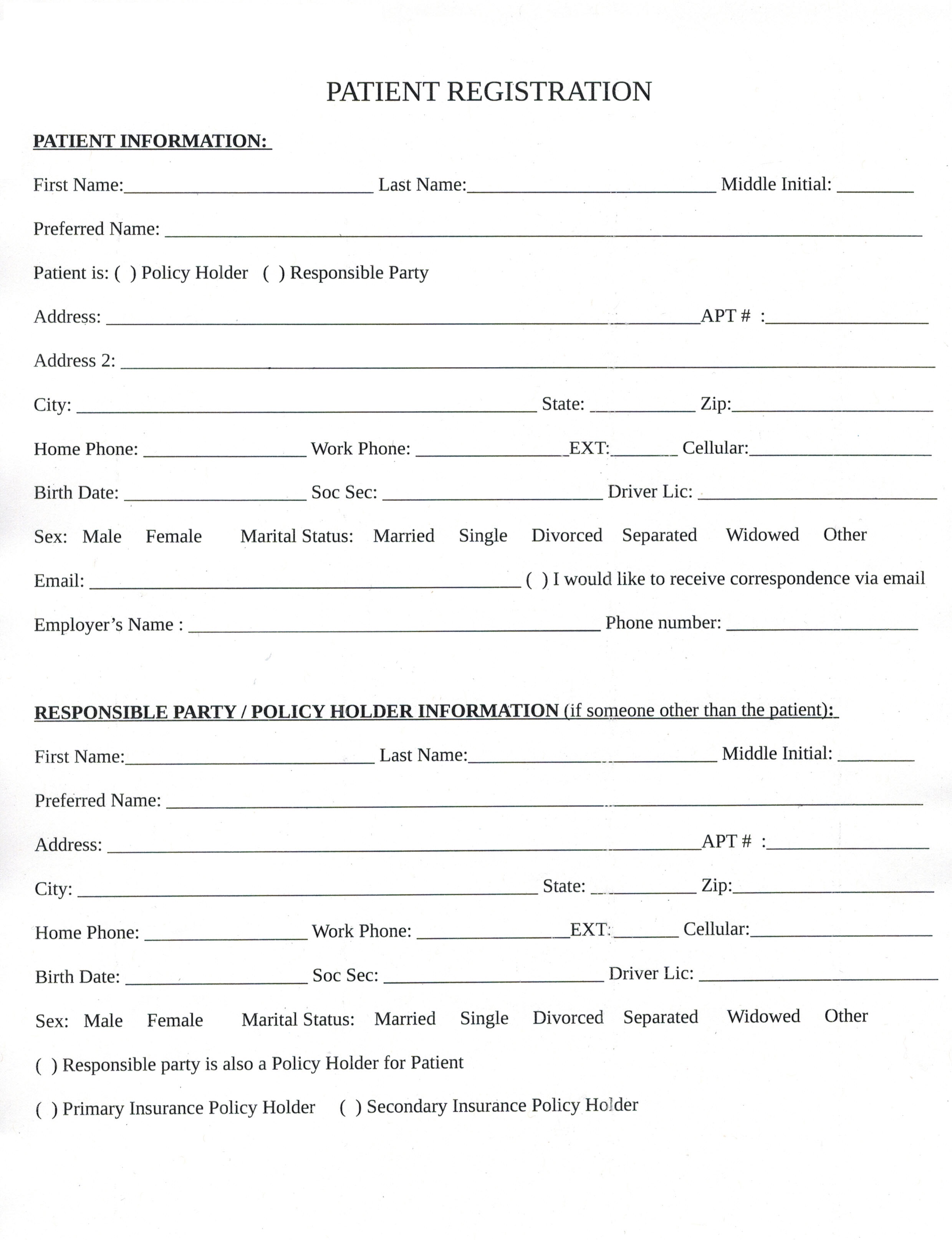
Payment arrangement form name of patient: Web dental history information i certify that i have read and understand the questions, above. Web download new dental patient forms to bring to your first dental appointment. Contact your local western dental with any questions! I acknowledge that my questions have been answered to my satisfaction. Save time and eliminate the hassles of filling out dental registration forms when you visit us. Contact your local brident with any questions! Date relationship to patient 1 patient information 2 dental insurance. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues. Web new patient registration form patient personal information title last, first address nickname city, state, zip email health care guardian name health care guardian phone # birth date marital status home # cell # emergency contact student school name referral type age sex work # drive lic emergency phone # ssn
I acknowledge that my questions have been answered to my satisfaction. Date relationship to patient 1 patient information 2 dental insurance. Save time and eliminate the hassles of filling out dental registration forms when you visit us. Patient registration form medical & dental history form privacy. Web new patient registration form patient personal information title last, first address nickname city, state, zip email health care guardian name health care guardian phone # birth date marital status home # cell # emergency contact student school name referral type age sex work # drive lic emergency phone # ssn I agree that i am responsible for all services rendered to the patient and that payment is. Web dental registration and history. Web download new dental patient forms to bring to your first dental appointment. We strive to make working with enable dental simple and easy. Contact your local western dental with any questions!
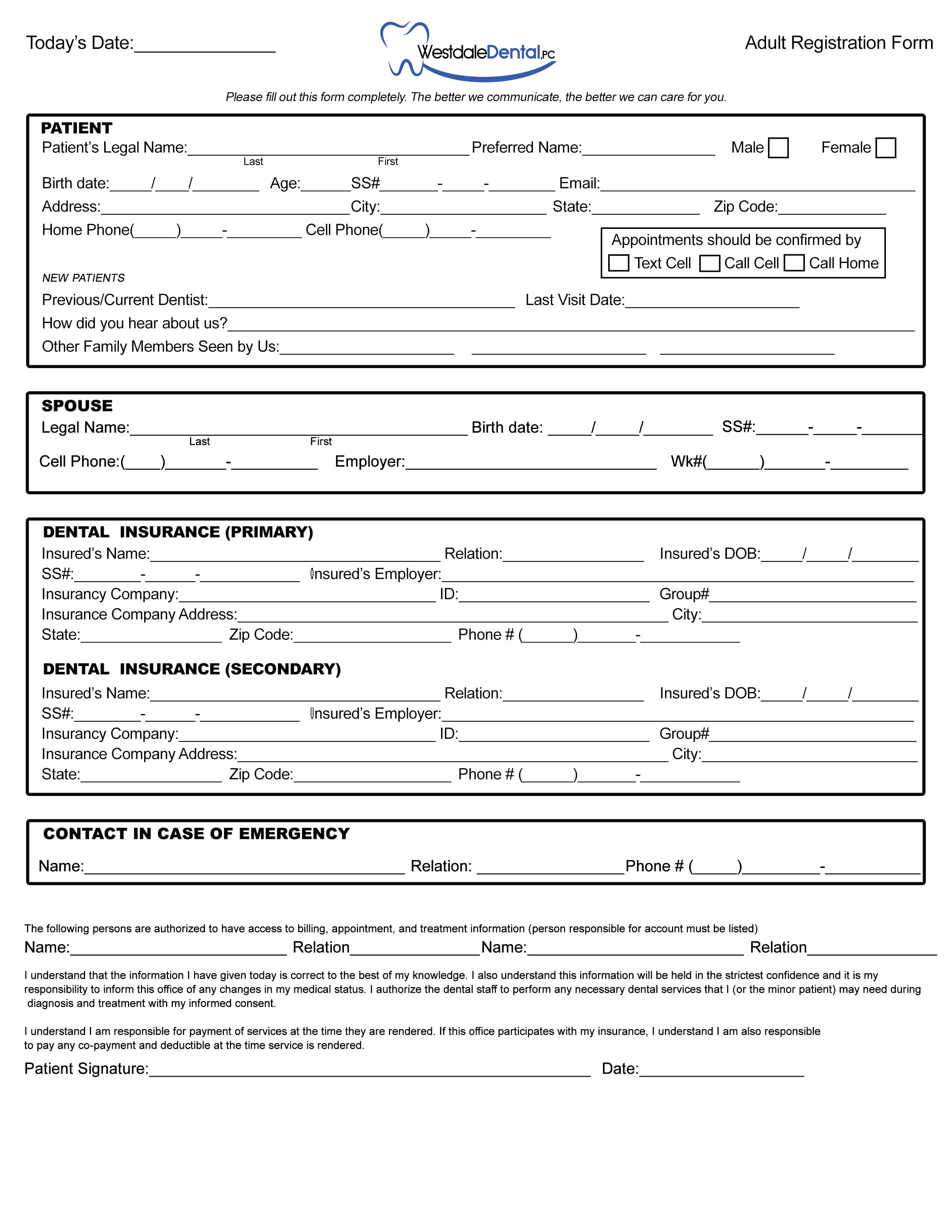
New Patient Forms Westdale Dental Cedar Rapids
For your convenience, simply download and print the forms below. We strive to make working with enable dental simple and easy. To get started, all new patients need to fill out a new patient registration form. Web download new dental patient forms to bring to your first dental appointment. Save time and eliminate the hassles of filling out dental registration.
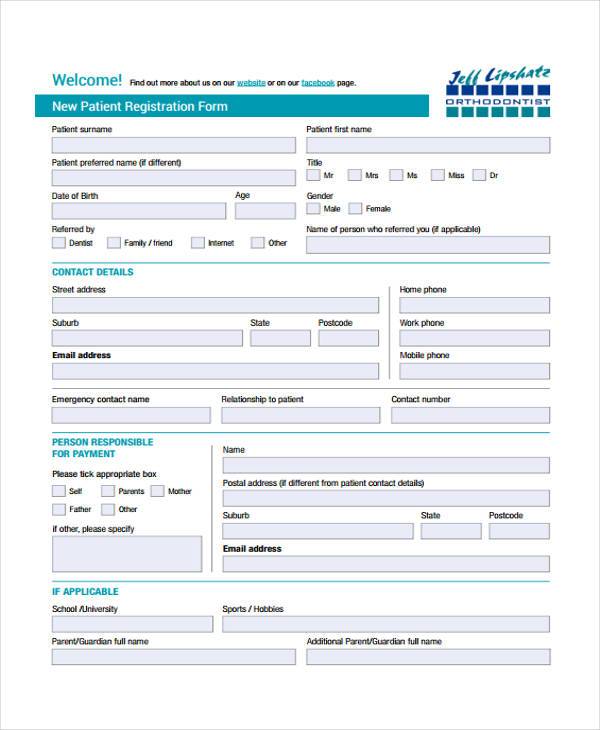
FREE 9+ Patient Registration Form Samples in PDF Excel MS Word
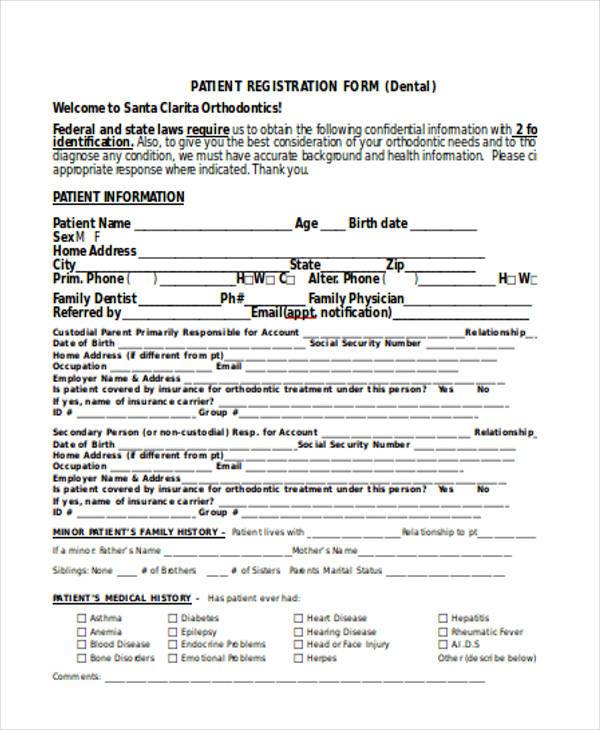
For your convenience, simply download and print the forms below. Physician’s name_____ date of last visit _____ have you ever used a bisphosphonate medication? Web dental registration and history. This can either be submitted via an online form, or you can also download the form as a pdf and submit to us directly. Common brand names are fosamax, actonel, atelvia,.
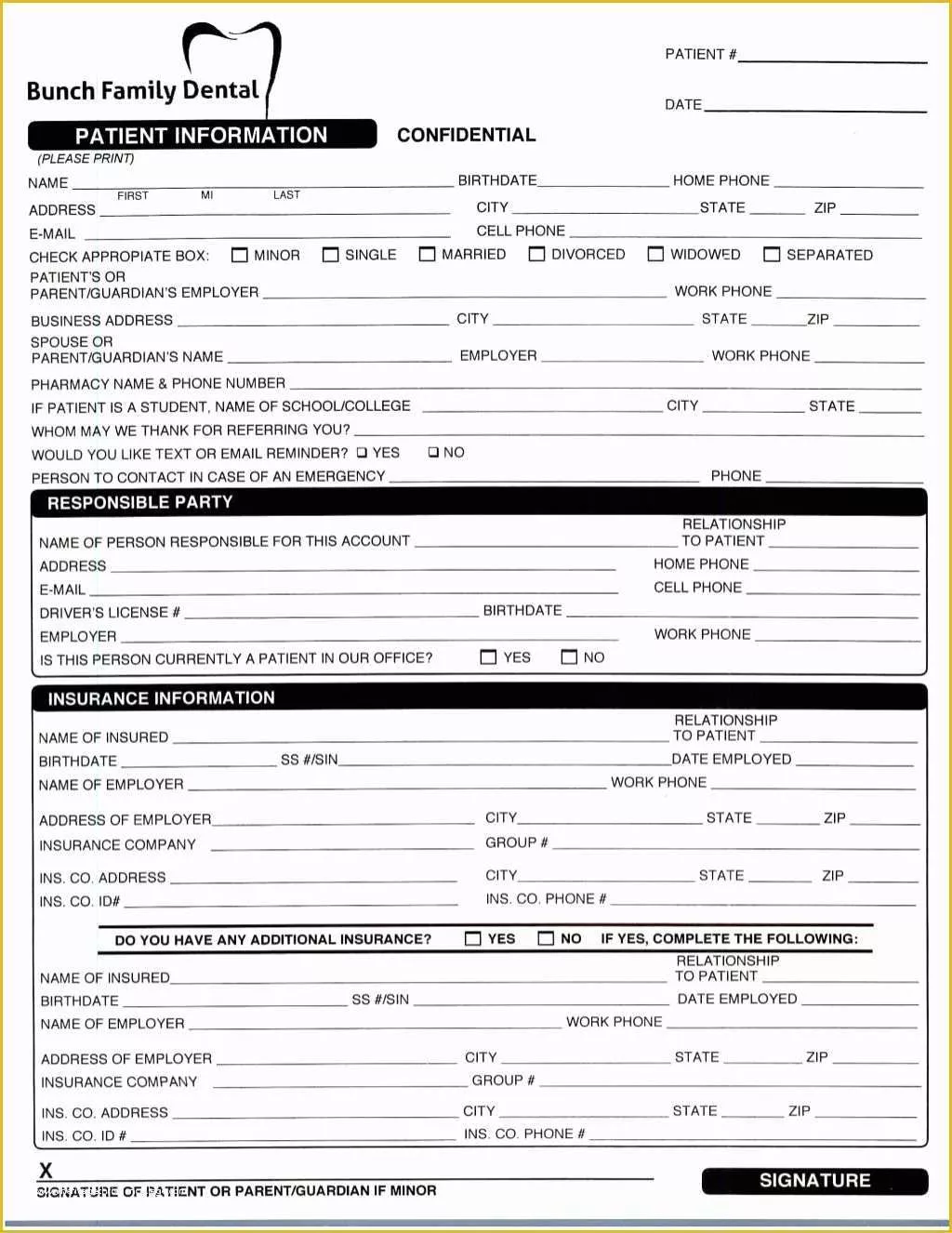
Free Patient Registration form Template Of New Patient Registration
Web new patient registration form patient personal information title last, first address nickname city, state, zip email health care guardian name health care guardian phone # birth date marital status home # cell # emergency contact student school name referral type age sex work # drive lic emergency phone # ssn For your convenience, simply download and print the forms.
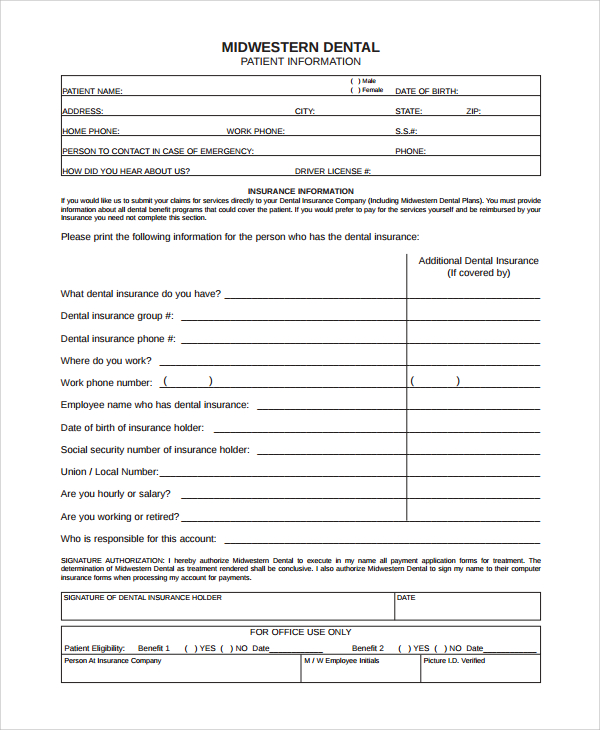
FREE 8+ Sample Patient Registration Forms in PDF MS Word
Web dental registration and history. We strive to make working with enable dental simple and easy. Save time and eliminate the hassles of filling out dental registration forms when you visit us. Web dental history information i certify that i have read and understand the questions, above. Contact your local brident with any questions!

Dental Patient Registration form Template Awesome Best S Of Medical
Date relationship to patient 1 patient information 2 dental insurance. Common brand names are fosamax, actonel, atelvia, didronel, boniva. Web new patient registration form patient personal information title last, first address nickname city, state, zip email health care guardian name health care guardian phone # birth date marital status home # cell # emergency contact student school name referral type.

Dental Medical History form Template Luxury 1960fp New Patient
Web dental registration and history. Contact your local brident with any questions! For your convenience, simply download and print the forms below. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues. Web take a little time now to save a lot.

Dental Patient Registration form Template Lovely 27 Of Dental New
Web download new dental patient forms to bring to your first dental appointment. The form is available in a digital, downloadable version or in print. To get started, all new patients need to fill out a new patient registration form. Physician’s name_____ date of last visit _____ have you ever used a bisphosphonate medication? We strive to make working with.
New Patient Forms Steeplechase Dental
Save time and eliminate the hassles of filling out dental registration forms when you visit us. I agree that i am responsible for all services rendered to the patient and that payment is. Web download new dental patient forms to bring to your first dental appointment. Contact your local brident with any questions! I acknowledge that my questions have been.
FREE 35+ Sample Registration Forms in MS Word
Common brand names are fosamax, actonel, atelvia, didronel, boniva. The form is available in a digital, downloadable version or in print. Web download new dental patient forms to bring to your first dental appointment. Date relationship to patient 1 patient information 2 dental insurance. Just complete before you visit, and remember the forms when you visit us for the first.
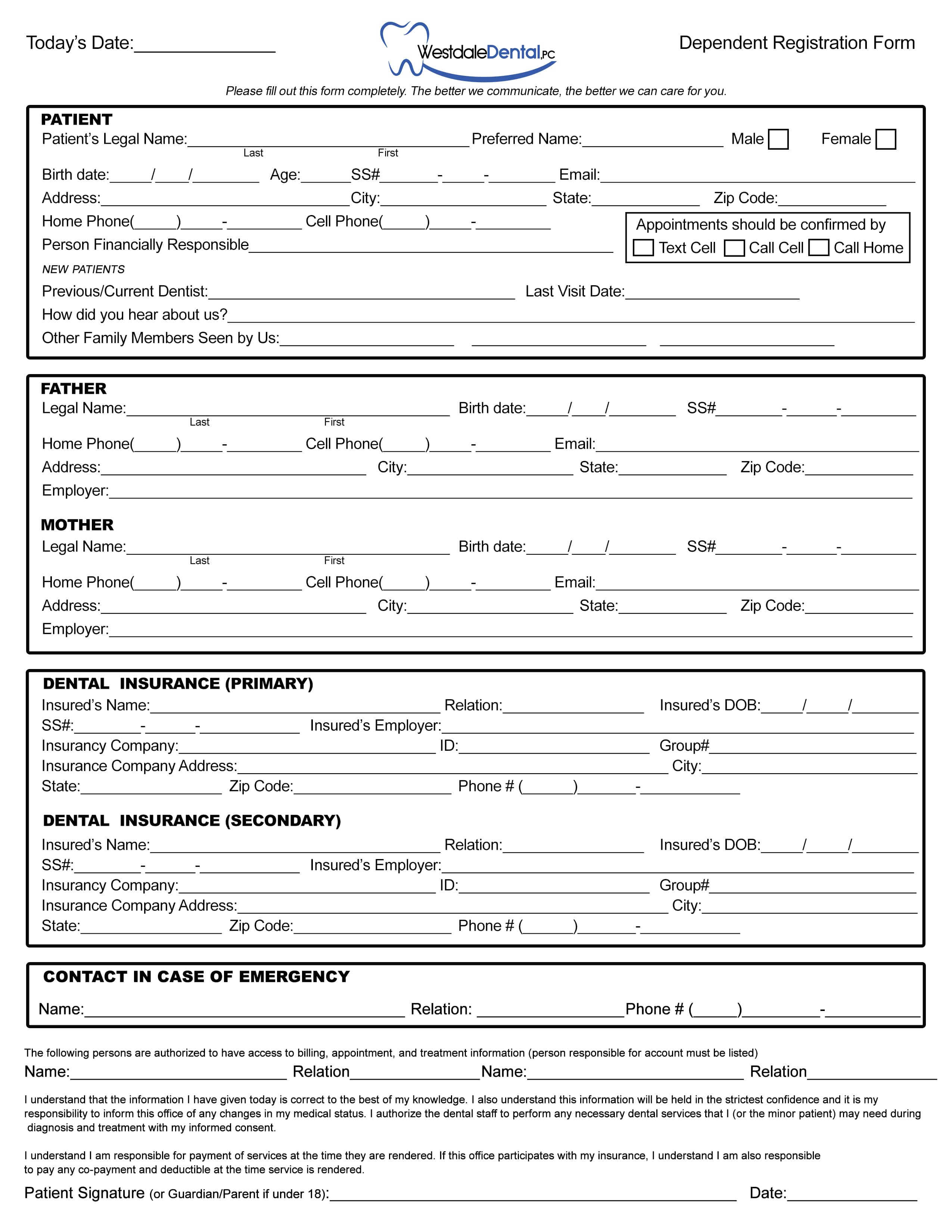
New Patient Forms Westdale Dental Cedar Rapids
Common brand names are fosamax, actonel, atelvia, didronel, boniva. This can either be submitted via an online form, or you can also download the form as a pdf and submit to us directly. Physician’s name_____ date of last visit _____ have you ever used a bisphosphonate medication? Save time and eliminate the hassles of filling out dental registration forms when.
Common Brand Names Are Fosamax, Actonel, Atelvia, Didronel, Boniva.
Web dental registration and history. To get started, all new patients need to fill out a new patient registration form. We strive to make working with enable dental simple and easy. Contact your local brident with any questions!
Payment Arrangement Form Name Of Patient:
Save time and eliminate the hassles of filling out dental registration forms when you visit us. Web download new dental patient forms to bring to your first dental appointment. For your convenience, simply download and print the forms below. Contact your local western dental with any questions!
Patient Registration Form Medical & Dental History Form Privacy.
Web download new dental patient forms to bring to your first dental appointment. Web new patient registration form patient personal information title last, first address nickname city, state, zip email health care guardian name health care guardian phone # birth date marital status home # cell # emergency contact student school name referral type age sex work # drive lic emergency phone # ssn I agree that i am responsible for all services rendered to the patient and that payment is. This can either be submitted via an online form, or you can also download the form as a pdf and submit to us directly.
Date Relationship To Patient 1 Patient Information 2 Dental Insurance.
Web take a little time now to save a lot later. I acknowledge that my questions have been answered to my satisfaction. The form is available in a digital, downloadable version or in print. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues.