Dexcom Prescription Form
Dexcom Prescription Form - Dexcom 8 7 6 5 4 3 2 1 poor glycemic control as evidenced by 72 hour cgms sensing trial. Pharmacare approval does not indicate that the. Web learn who is able to participate and how to apply for the dexcom patient assistance program. This fillable cmn form can also. Information will only be used and disclosed in accordance. Web changes to form must be initialed and dated by prescriber. Web dexcom prior authorization request form (page 1 of 2) do not copy for future use. If you pick up your dexcom g6 supplies up at a pharmacy, all you need to do is get a dexcom g7 prescription from your doctor and continue through. Our standard response time for prescription drug coverage requests is. Web ** the dexcom g6 requires a separate prescription and is necessary to use omnipod 5 in automated mode.
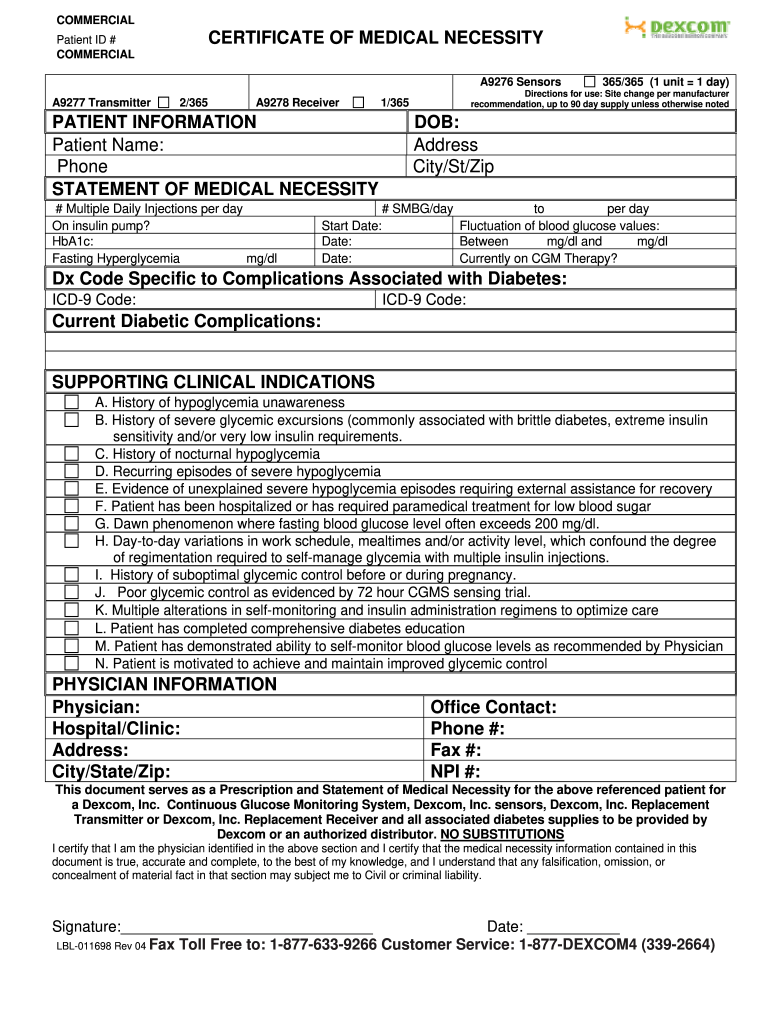
Web if pharmacare approves this special authority request, approval is granted solely for the purpose of covering prescription costs. Web changes to form must be initialed and dated by prescriber. Web use this dexcom certificate of medical necessity (cmn) to document medical necessity of dexcom g6 cgm for your commercially insured patients. Web ** the dexcom g6 requires a separate prescription and is necessary to use omnipod 5 in automated mode. Forms are updated frequently and may have barcodes. If your doctor confirms your. Financial assistance programs may be available have your patients. Dexcom 8 7 6 5 4 3 2 1 poor glycemic control as evidenced by 72 hour cgms sensing trial. Either dexcom, or a service. Please provide your treating healthcare provider's information below to obtain a sample.
Information will only be used and disclosed in accordance. Date of last visit (must be within 6 months of this order): If your doctor confirms your. Web changes to form must be initialed and dated by prescriber. This fillable cmn form can also. If you pick up your dexcom g6 supplies up at a pharmacy, all you need to do is get a dexcom g7 prescription from your doctor and continue through. Pharmacare approval does not indicate that the. Web dexcom prior authorization request form (page 1 of 2) do not copy for future use. Dexcom g6 is covered by many provincial healthcare. Please provide your treating healthcare provider's information below to obtain a sample.
2004 Form LBL011698 Fill Online, Printable, Fillable, Blank
Dexcom g6 is covered by many provincial healthcare. 6340 sequence drive san diego, ca 92121 barcode: Information will only be used and disclosed in accordance. Dexcom 8 7 6 5 4 3 2 1 poor glycemic control as evidenced by 72 hour cgms sensing trial. Web if pharmacare approves this special authority request, approval is granted solely for the purpose.

Advanced Cheat Sheet.. Diabetes care, Diabetes information
Getting your diabetes patients started on dexcom g6 is easy using the steps below. Web covered by medicare‡ more medicare patients are eligible for cgm than ever before, and no other cgm system is less expensive for medicare patients than dexcom cgm.§ get. Date of last visit (must be within 6 months of this order): If you pick up your.

Inc Fill and Sign Printable Template Online US Legal Forms
Web covered by medicare‡ more medicare patients are eligible for cgm than ever before, and no other cgm system is less expensive for medicare patients than dexcom cgm.§ get. If you pick up your dexcom g6 supplies up at a pharmacy, all you need to do is get a dexcom g7 prescription from your doctor and continue through. Our standard.

Prescribe Today G6 CGM System Prescription Healthcare
Web if pharmacare approves this special authority request, approval is granted solely for the purpose of covering prescription costs. Date of last visit (must be within 6 months of this order): Recognizes that medical information is confidential and will maintain the privacy of your medical information. Web learn who is able to participate and how to apply for the dexcom.
Prescribe Today G6 CGM System Prescription Healthcare
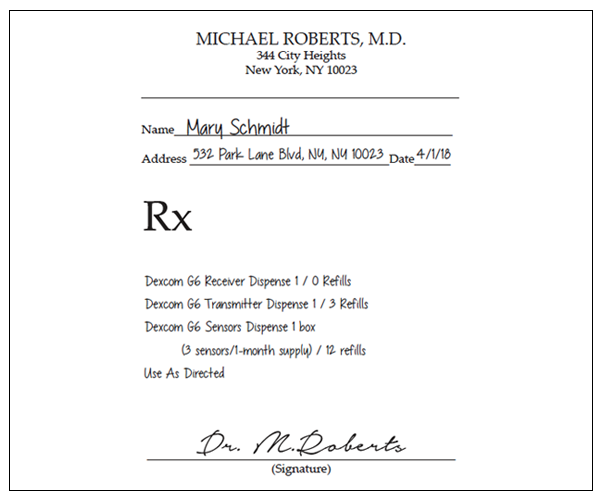
Web current dexcom g6 users. Please provide your treating healthcare provider's information below to obtain a sample. Dexcom 8 7 6 5 4 3 2 1 poor glycemic control as evidenced by 72 hour cgms sensing trial. Web dexcom cgm systems are available by prescription. If your doctor confirms your.

G6 Prescription Rx Form World OSCAR
Web learn who is able to participate and how to apply for the dexcom patient assistance program. Web dexcom cgm systems are available by prescription. Our standard response time for prescription drug coverage requests is. Web ** the dexcom g6 requires a separate prescription and is necessary to use omnipod 5 in automated mode. Web use this dexcom certificate of.

Is this average price paid for a 3 month supply? G6
Web learn who is able to participate and how to apply for the dexcom patient assistance program. If you pick up your dexcom g6 supplies up at a pharmacy, all you need to do is get a dexcom g7 prescription from your doctor and continue through. Pharmacare approval does not indicate that the. Information will only be used and disclosed.

Prescribe Today G6 CGM System Prescription Healthcare
Find additional dexcom g6 prescribing information for healthcare providers below, such as commercial and medicare coverage. Web ** the dexcom g6 requires a separate prescription and is necessary to use omnipod 5 in automated mode. Web current dexcom g6 users. Forms are updated frequently and may have barcodes. Web use this dexcom certificate of medical necessity (cmn) to document medical.

Posts Strong Revenue, Stock Up 70 San Diego Business Journal
Getting your diabetes patients started on dexcom g6 is easy using the steps below. 6340 sequence drive san diego, ca 92121 barcode: If you pick up your dexcom g6 supplies up at a pharmacy, all you need to do is get a dexcom g7 prescription from your doctor and continue through. Web use this dexcom certificate of medical necessity (cmn).

All About the G6 Continuous Glucose Monitor
Pharmacare approval does not indicate that the. Our standard response time for prescription drug coverage requests is. Web changes to form must be initialed and dated by prescriber. Web ** the dexcom g6 requires a separate prescription and is necessary to use omnipod 5 in automated mode. Web use this dexcom certificate of medical necessity (cmn) to document medical necessity.
This Fillable Cmn Form Can Also.
Financial assistance programs may be available have your patients. Forms are updated frequently and may have barcodes. Information will only be used and disclosed in accordance. Web dexcom cgm systems are available by prescription.
Recognizes That Medical Information Is Confidential And Will Maintain The Privacy Of Your Medical Information.
Web use this dexcom certificate of medical necessity (cmn) to document medical necessity of dexcom g6 cgm for your commercially insured patients. Web changes to form must be initialed and dated by prescriber. Find additional dexcom g6 prescribing information for healthcare providers below, such as commercial and medicare coverage. Dexcom 8 7 6 5 4 3 2 1 poor glycemic control as evidenced by 72 hour cgms sensing trial.
Web Current Dexcom G6 Users.
Getting your diabetes patients started on dexcom g6 is easy using the steps below. 6340 sequence drive san diego, ca 92121 barcode: If you pick up your dexcom g6 supplies up at a pharmacy, all you need to do is get a dexcom g7 prescription from your doctor and continue through. Our standard response time for prescription drug coverage requests is.
Pharmacare Approval Does Not Indicate That The.
Either dexcom, or a service. Web learn who is able to participate and how to apply for the dexcom patient assistance program. Please provide your treating healthcare provider's information below to obtain a sample. Date of last visit (must be within 6 months of this order):