Doh-4359 Form
Doh-4359 Form - Sign it in a few clicks draw your signature, type it, upload its image, or use your mobile device as a signature pad. Enter the patient’s height and weight. For the condition(s) requiring personal care: Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. Patient identifying information (use additional paper if necessary) 2. Edit your doh 4359 template online type text, add images, blackout confidential details, add comments, highlights and more. The best place to get access to and use this form is here. Mds, dos, nps, pas, and specialist assistants. Patient identifying information (use additional paper if necessary) 2. Save or instantly send your ready documents.
Practitioners able to sign the nyia po forms include the following provider types: Web the doh 4359 form is a form that all hospitals must submit to the department of health, detailing deaths and serious injuries during surgery. For the condition(s) requiring personal care: Edit your doh 4359 template online type text, add images, blackout confidential details, add comments, highlights and more. Share your form with others send doh 4359 via email, link, or fax. Easily fill out pdf blank, edit, and sign them. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. Patient identifying information (use additional paper if necessary) 2. Sign it in a few clicks draw your signature, type it, upload its image, or use your mobile device as a signature pad. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form.
Patient identifying information (use additional paper if necessary) 2. • primary and secondary diagnosis. Patient identifying information (use additional paper if necessary) 2. Enter the patient’s height and weight. The best place to get access to and use this form is here. Save or instantly send your ready documents. For the condition(s) requiring personal care: Easily fill out pdf blank, edit, and sign them. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. Web the doh 4359 form is a form that all hospitals must submit to the department of health, detailing deaths and serious injuries during surgery.
Form Doh30 Adoptee Registration Form Edit, Fill, Sign Online
Save or instantly send your ready documents. Patient identifying information (use additional paper if necessary) 2. Easily fill out pdf blank, edit, and sign them. Patient identifying information (use additional paper if necessary) 2. Share your form with others send doh 4359 via email, link, or fax.
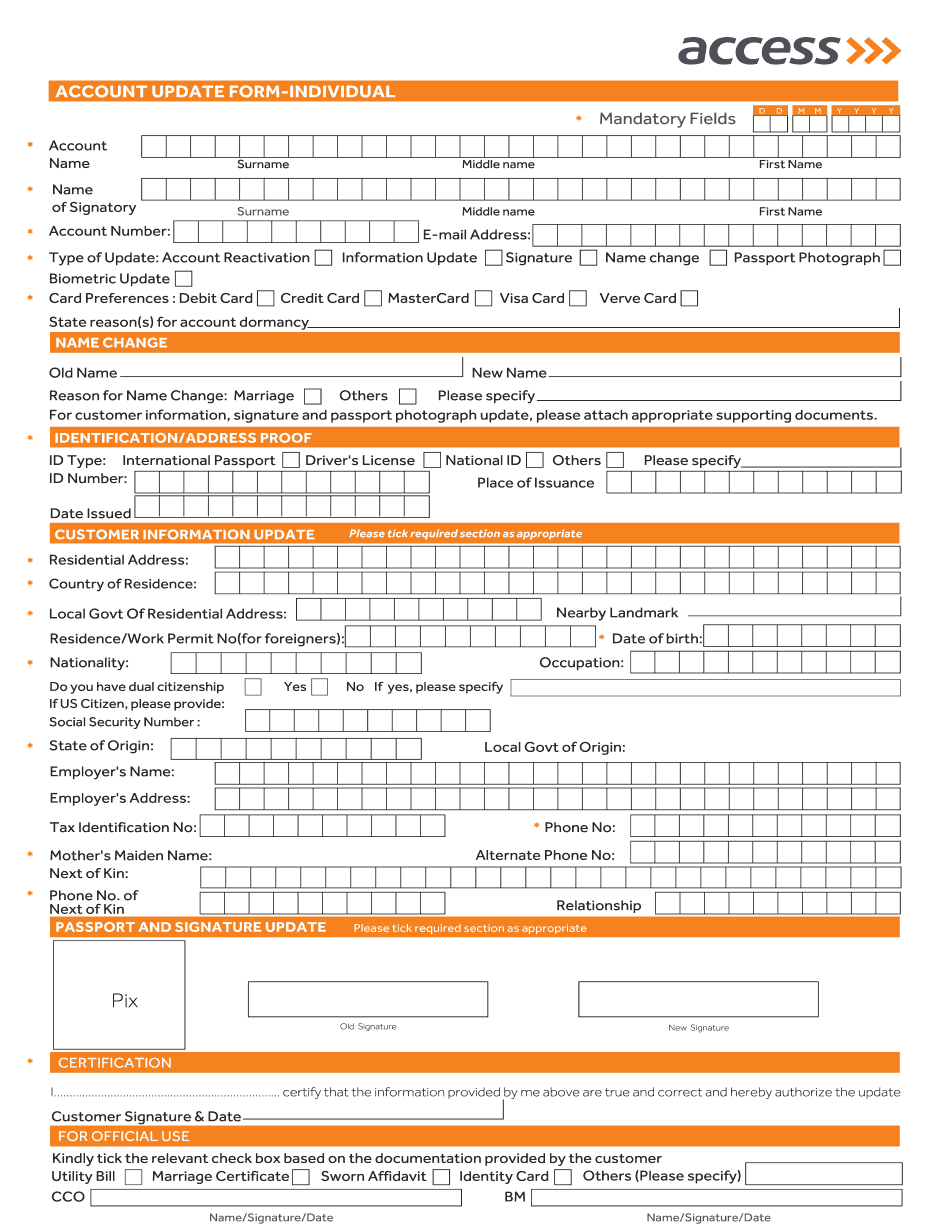
Create Fillable Access Bank Account Update Form And Keep Things Organized
Patient identifying information (use additional paper if necessary) 2. The best place to get access to and use this form is here. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. Patient identifying information (use additional paper if necessary) 2. Enter the patient’s height.
Doh 4359 Form ≡ Fill Out Printable PDF Forms Online
The best place to get access to and use this form is here. • primary and secondary diagnosis. Practitioners able to sign the nyia po forms include the following provider types: Edit your doh 4359 template online type text, add images, blackout confidential details, add comments, highlights and more. Patient identifying information (use additional paper if necessary) 2.
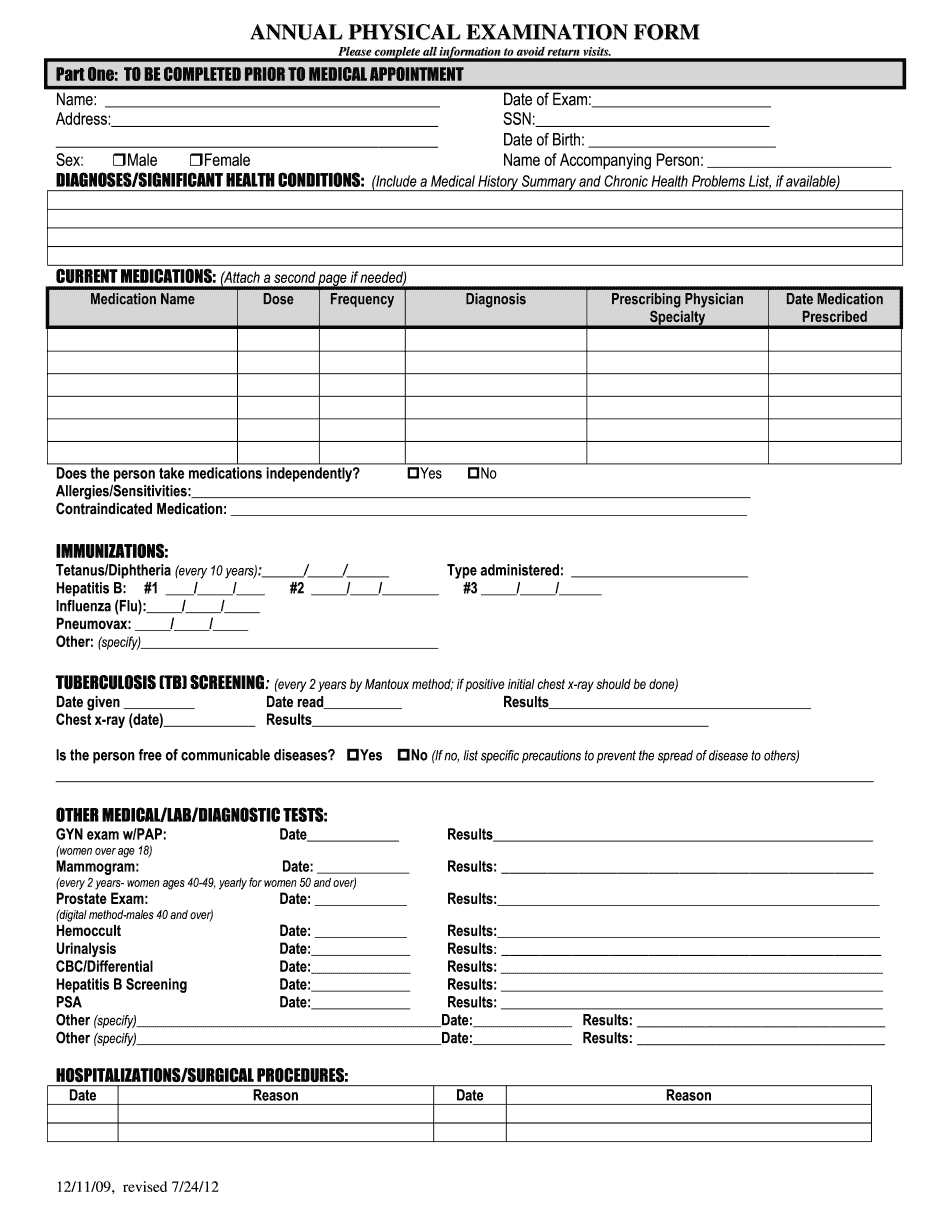
Edit Document Basic Physical Exam Form With Us Fastly, Easyly, And Securely
Share your form with others send doh 4359 via email, link, or fax. Save or instantly send your ready documents. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. Sign it in a few clicks draw your signature, type it, upload its image, or.
DA Form 4359 Download Fillable PDF or Fill Online Authorization for
Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. For the condition(s) requiring personal care: Save or instantly send your ready documents. Easily fill out pdf blank, edit, and sign them. Web the doh 4359 form is a form that all hospitals must submit.

600569 UK Doherty Baxter Cycle
Web the doh 4359 form is a form that all hospitals must submit to the department of health, detailing deaths and serious injuries during surgery. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. Patient identifying information (use additional paper if necessary) 2. For.
Form DOH4081 Download Printable PDF or Fill Online Initial Limited
• primary and secondary diagnosis. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. Mds, dos, nps, pas, and specialist assistants. Patient identifying information (use additional paper if necessary) 2. Sign it in a few clicks draw your signature, type it, upload its image,.

Doh 4359 Fill Online, Printable, Fillable, Blank pdfFiller
Sign it in a few clicks draw your signature, type it, upload its image, or use your mobile device as a signature pad. Save or instantly send your ready documents. • primary and secondary diagnosis. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form..
Captain D's Application Pdf Fill Out and Sign Printable PDF Template
Share your form with others send doh 4359 via email, link, or fax. Save or instantly send your ready documents. Edit your doh 4359 template online type text, add images, blackout confidential details, add comments, highlights and more. Mds, dos, nps, pas, and specialist assistants. Sign it in a few clicks draw your signature, type it, upload its image, or.

MP1006 Lesson 6
Practitioners able to sign the nyia po forms include the following provider types: • primary and secondary diagnosis. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. Patient identifying information (use additional paper if necessary) 2. Indicate n/a if an item does not apply.
Practitioners Able To Sign The Nyia Po Forms Include The Following Provider Types:
The best place to get access to and use this form is here. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. • primary and secondary diagnosis. Edit your doh 4359 template online type text, add images, blackout confidential details, add comments, highlights and more.
Enter The Patient’s Height And Weight.
Easily fill out pdf blank, edit, and sign them. Mds, dos, nps, pas, and specialist assistants. Patient identifying information (use additional paper if necessary) 2. Share your form with others send doh 4359 via email, link, or fax.
Save Or Instantly Send Your Ready Documents.
Patient identifying information (use additional paper if necessary) 2. For the condition(s) requiring personal care: Sign it in a few clicks draw your signature, type it, upload its image, or use your mobile device as a signature pad. Web the doh 4359 form is a form that all hospitals must submit to the department of health, detailing deaths and serious injuries during surgery.
Indicate N/A If An Item Does Not Apply To This Patient Or Unk If The Requested Information Is Unknown To The Physician Signing This Form.
Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form.