Express Scripts Formulary Exception Form
Express Scripts Formulary Exception Form - Web download the form and mail it to us. To make a bulk request for electronic data, please download this form. Web once a decision has been made, express scripts will send a letter to the physician’s office and the member regarding the decision of the coverage determination. Express scripts, part of cigna’s evernorth company, has released its 2022 list of. Web please call us at 800.753.2851 to submit a verbal prior authorization request if you are unable to use electronic prior authorization. Web how do i find local pharmacies covered by my plan? Web crp1905_0262 y0046_ot48610a_c type of coverage determination request i need a drug that is not on the plan’s*list of covered drugs (formulary exception). Our pharmacy benefit manager, express scripts,. (1) formulary or preferred drug(s) tried and results of drug. Web third party request for electronic protected health information.
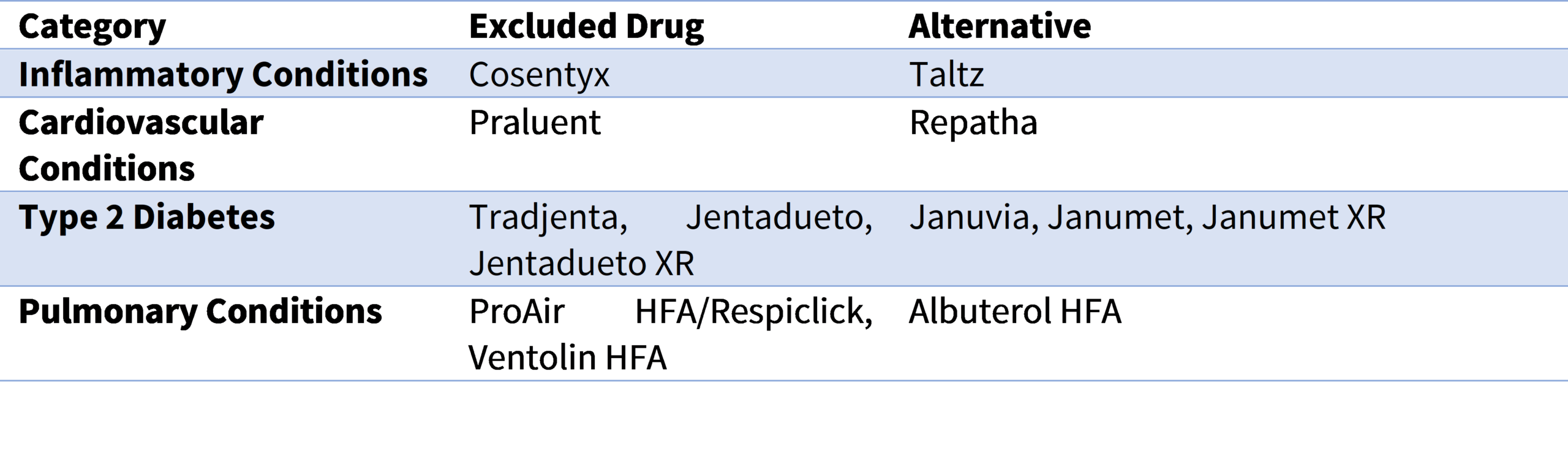
Web ☐ request for formulary tier exception specify below if not noted in the drug history section earlier on the form: Web four products on the preferred list this year will be excluded next year. Web express scripts is the pharmacy benefit manager for mutual of omaha rx and will be providing this service on behalf of mutual of omaha rx. Complete the form and send it to. If the formulary exception is denied, the patient or their representative may appeal the decision. Web once a decision has been made, express scripts will send a letter to the physician’s office and the member regarding the decision of the coverage determination. Web how do i find local pharmacies covered by my plan? To make a bulk request for electronic data, please download this form. See the section “how do i request an. Web crp1905_0262 y0046_ot48610a_c type of coverage determination request i need a drug that is not on the plan’s*list of covered drugs (formulary exception).
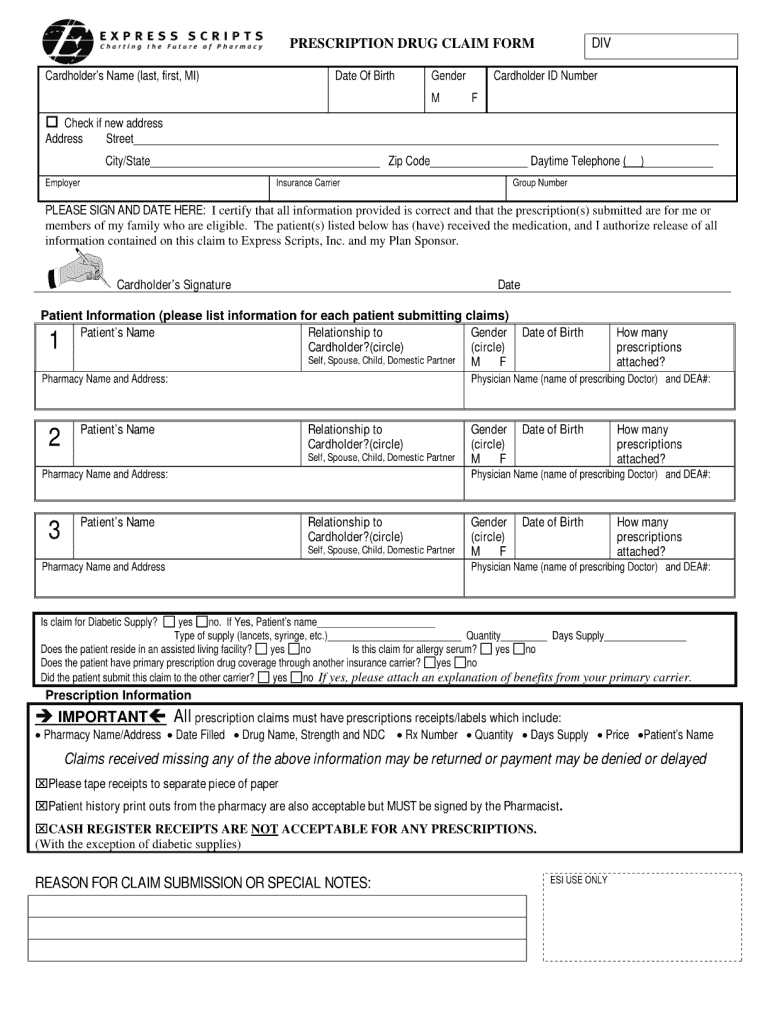
This document contains information about some of. Our pharmacy benefit manager, express scripts,. If i have other health insurance (ohi), can i use tricare retail network pharmacies? How do i find out if the medication i need. Web once a decision has been made, express scripts will send a letter to the physician’s office and the member regarding the decision of the coverage determination. Web four products on the preferred list this year will be excluded next year. Register now we make it easy to share information get your written prescriptions to us by using our mail order form. Web log in don't have an account? Web express scripts is the pharmacy benefit manager for mutual of omaha rx and will be providing this service on behalf of mutual of omaha rx. Web download the form and mail it to us.
How to Get Prescription Refill Home
Web four products on the preferred list this year will be excluded next year. Register now we make it easy to share information get your written prescriptions to us by using our mail order form. Web prior authorization and formulary exception requests may be submitted for review. How do i find out if the medication i need. You can ask.

PDF Prescription coverage in Canada a review of the
Follow these links or log in to find the form. This document contains information about some of. To make a bulk request for electronic data, please download this form. Web once a decision has been made, express scripts will send a letter to the physician’s office and the member regarding the decision of the coverage determination. Complete the form and.
Express Scripts Fax Forms for Physicians Prior Authorization Fill Out
You can ask us to cover your. Included below is the information you need to submit a request on behalf of your. How do i find out if the medication i need. Web pharmacy authorizations & formulary exceptions authorizations for targeted medications, step therapy medications and formulary exception requests. Web an exception to the formulary exclusion.
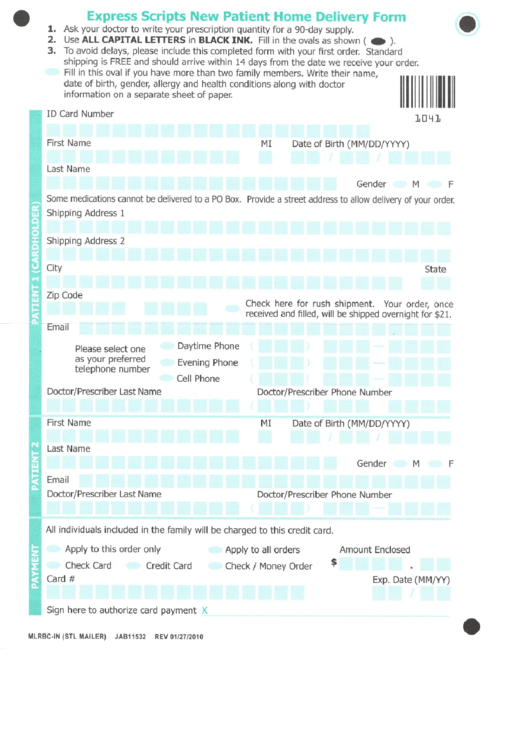
Express Scripts Mail Order Form printable pdf download
Web crp1905_0262 y0046_ot48610a_c type of coverage determination request i need a drug that is not on the plan’s*list of covered drugs (formulary exception). Web please call us at 800.753.2851 to submit a verbal prior authorization request if you are unable to use electronic prior authorization. A drug that has the same. Web download the form and mail it to us..

Express Scripts Cuts 48 Drugs from 2019 Formulary
If i have other health insurance (ohi), can i use tricare retail network pharmacies? Web download the form and mail it to us. You can ask us to make an exception to these restrictions or limits. Follow these links or log in to find the form. Web an exception to the formulary exclusion.
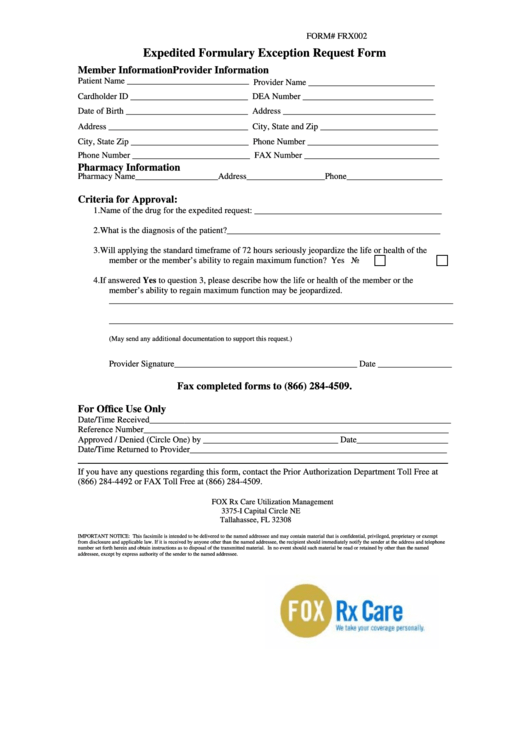
Form Frx002 Expedited Formulary Exception Request Form printable pdf
(1) formulary or preferred drug(s) tried and results of drug. Web third party request for electronic protected health information. Register now we make it easy to share information get your written prescriptions to us by using our mail order form. Web log in don't have an account? If i have other health insurance (ohi), can i use tricare retail network.

Express Scripts offers lowcost alternative to Turing's 750 per pill
Web express scripts medicare (pdp) 2023 formulary (list of covered drugs) please read: Web how do i find local pharmacies covered by my plan? Prior authorization criteria is available upon. A drug that has the same. You can ask us to make an exception to these restrictions or limits.
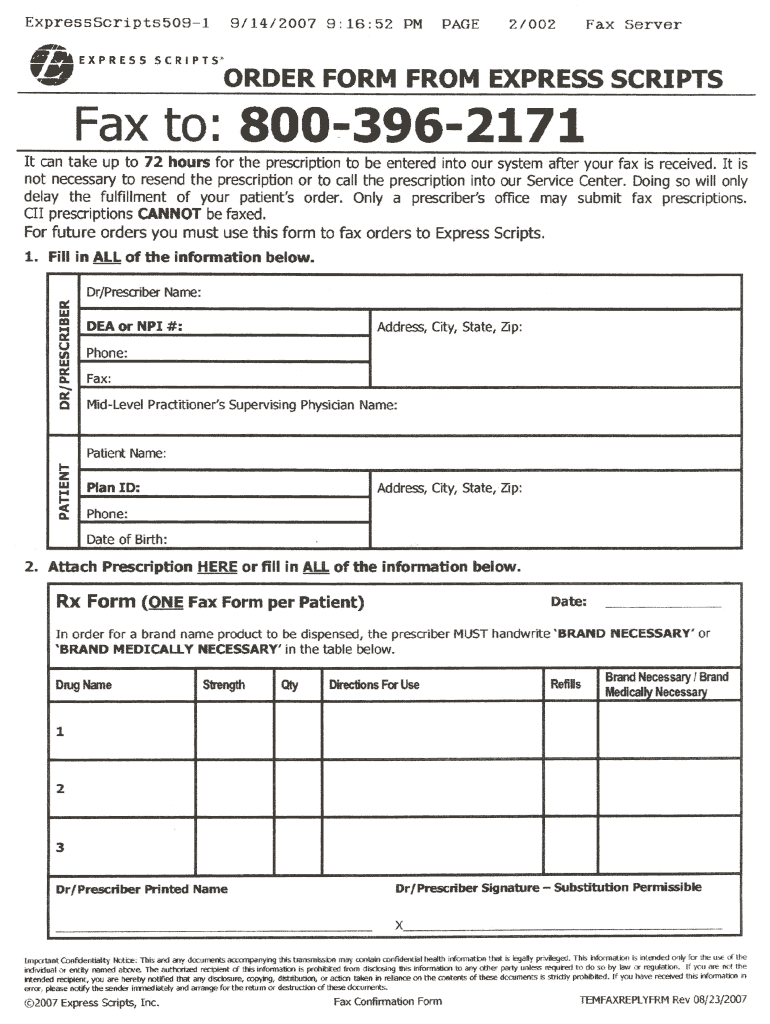
Order Form from Express Scripts 20072021 Fill and Sign Printable
You can ask us to cover your. Web four products on the preferred list this year will be excluded next year. You can ask us to make an exception to these restrictions or limits. Web how do i find local pharmacies covered by my plan? Web express scripts medicare (pdp) 2023 formulary (list of covered drugs) please read:

Express Scripts forms Elegant This
Our pharmacy benefit manager, express scripts,. A drug that has the same. Web third party request for electronic protected health information. Web once a decision has been made, express scripts will send a letter to the physician’s office and the member regarding the decision of the coverage determination. Web please call us at 800.753.2851 to submit a verbal prior authorization.
Pharmaceutical Strategies Group PSG 2021 Express Scripts
Included below is the information you need to submit a request on behalf of your. Web prior authorization and formulary exception requests may be submitted for review. Our pharmacy benefit manager, express scripts,. Prior authorization criteria is available upon. How do i find out if the medication i need.
If I Have Other Health Insurance (Ohi), Can I Use Tricare Retail Network Pharmacies?
Web download the form and mail it to us. Express scripts, part of cigna’s evernorth company, has released its 2022 list of. This document contains information about some of. Web please call us at 800.753.2851 to submit a verbal prior authorization request if you are unable to use electronic prior authorization.
Web Prior Authorization And Formulary Exception Requests May Be Submitted For Review.
Prior authorization criteria is available upon. Complete the form and send it to. Web crp1905_0262 y0046_ot48610a_c type of coverage determination request i need a drug that is not on the plan’s*list of covered drugs (formulary exception). Web log in don't have an account?
See The Section “How Do I Request An.
Register now we make it easy to share information get your written prescriptions to us by using our mail order form. Web once a decision has been made, express scripts will send a letter to the physician’s office and the member regarding the decision of the coverage determination. Follow these links or log in to find the form. You can ask us to cover your.
(1) Formulary Or Preferred Drug(S) Tried And Results Of Drug.
Web four products on the preferred list this year will be excluded next year. Web third party request for electronic protected health information. Web pharmacy authorizations & formulary exceptions authorizations for targeted medications, step therapy medications and formulary exception requests. Web ☐ request for formulary tier exception specify below if not noted in the drug history section earlier on the form: