Form 110 Workers Compensation
Form 110 Workers Compensation - Web online rate comparisons of all workers' compensation insurers in missouri. 1 copy for the workers’. An employer, or a third party designated by the employer, shall record any injury or illness incurred by one of its employees in the. Web form (form 110) when to fill out this employee’s claim form this employee claim form should be completed whenever you believe you are not. Web deu form 110 (rev. Report your injury immediately to your employer or supervisor. Please fill out the form completely and accurately. You will need 3 copies of this form and all other materials: 1 copy for the dia; Web any part of your claim and refuses to pay the compensation that you believe you are entitled.
Web any part of your claim and refuses to pay the compensation that you believe you are entitled. Web missouri employers are required to carry workers’ compensation insurance if they have five or more employees. 10/2013) declaration of service i. You will need 3 copies of this form and all other materials: Web permanent disability rating determination. Web form (form 110) when to fill out this employee’s claim form this employee claim form should be completed whenever you believe you are not. Failure to report your injury to your employer within 30 days may jeopardize. Missouri employers involved in the construction. 1 copy for the dia; Web report your injury immediately.
Web any part of your claim and refuses to pay the compensation that you believe you are entitled. Web form (form 110) when to fill out this employee’s claim form this employee claim form should be completed whenever you believe you are not. Web permanent disability rating determination. Failure to report your injury to your employer within 30 days may jeopardize. 1 copy for the dia; An employer, or a third party designated by the employer, shall record any injury or illness incurred by one of its employees in the. Report your injury immediately to your employer or supervisor. State of california department of. Notice of options following disability rating (deu form 110). You should complete this form when you believe you are not getting all of the.

2019 AU 110 Form Fill Online, Printable, Fillable, Blank pdfFiller
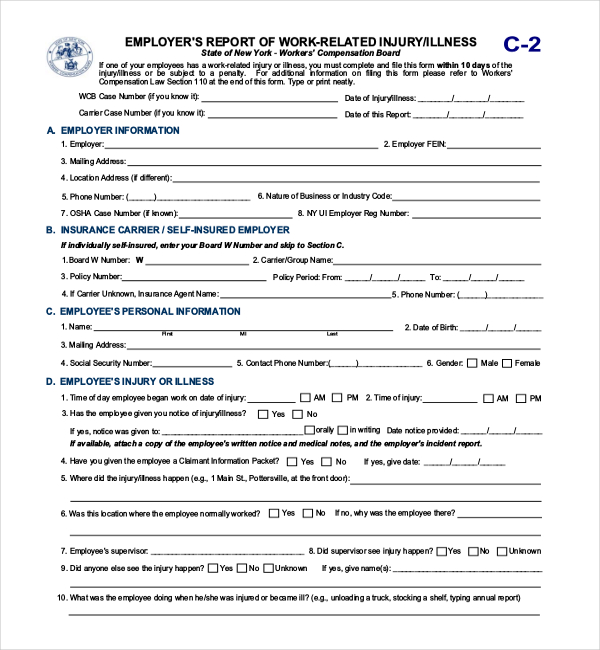
An employer, or a third party designated by the employer, shall record any injury or illness incurred by one of its employees in the. Record and report of injuries by employers. 10/2013) declaration of service i. Missouri employers involved in the construction. You will need 3 copies of this form and all other materials:
FREE 13+ Sample Workers Compensation Forms in PDF XLS Word
An employer, or a third party designated by the employer, shall record any injury or illness incurred by one of its employees in the. Web missouri employers are required to carry workers’ compensation insurance if they have five or more employees. Notice of options following disability rating (deu form 110). Failure to report your injury to your employer within 30.

Workers Compensation Waiver Form Texas Universal Network
1 copy for the dia; Web deu form 110 (rev. 1 copy for the workers’. Missouri employers involved in the construction. 1 copy for the workers’.
How To Fill Out A Workers Compensation Form Form Resume Examples
Failure to report your injury to your employer within 30 days may jeopardize. An employer, or a third party designated by the employer, shall record any injury or illness incurred by one of its employees in the. 1 copy for the workers’. You should complete this form when you believe you are not getting all of the. Missouri employers involved.

Certificate Of Attestation Of Exemption Nys Workers Compensation
Failure to report your injury to your employer within 30 days may jeopardize. 10/2013) declaration of service i. Web form (form 110) when to fill out this employee’s claim form this employee claim form should be completed whenever you believe you are not. Web report your injury immediately. An employer, or a third party designated by the employer, shall record.
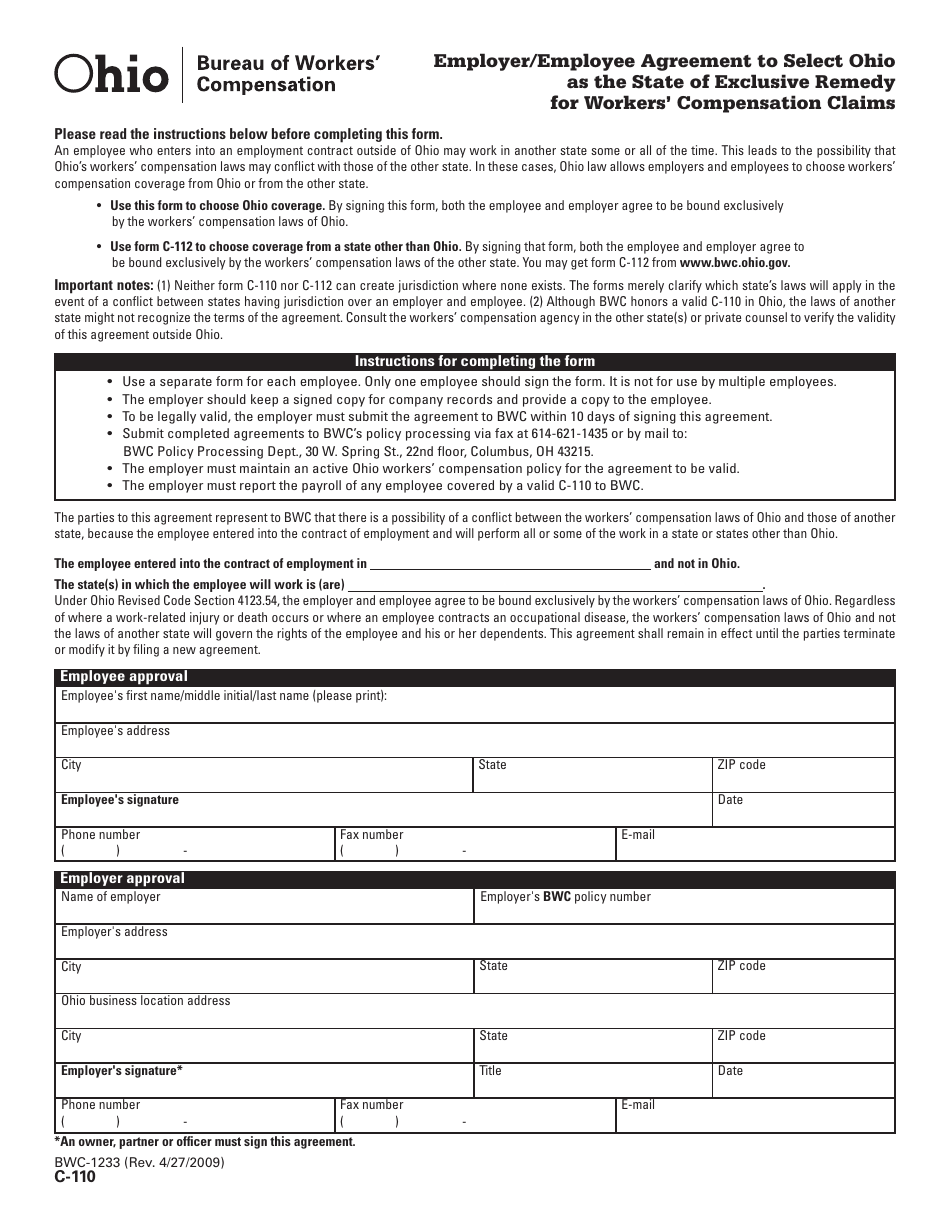
Form C110 (BWC1233) Download Printable PDF or Fill Online Employer
Web deu form 110 (rev. You will need 3 copies of this form and all other materials: 1 copy for the dia; 1 copy for the workers’. 10/2013) declaration of service i.
Nevada Workers Compensation Waiver Form Form Resume Examples
An employer, or a third party designated by the employer, shall record any injury or illness incurred by one of its employees in the. Please fill out the form completely and accurately. Report your injury immediately to your employer or supervisor. Web online rate comparisons of all workers' compensation insurers in missouri. Record and report of injuries by employers.
How To Fill Out A Workers Compensation Form Form Resume Examples
1 copy for the dia; Web deu form 110 (rev. 10/2013) declaration of service i. State of california department of. An employer, or a third party designated by the employer, shall record any injury or illness incurred by one of its employees in the.

Workers' Compensation Claim Form California Free Download
Report your injury immediately to your employer or supervisor. Record and report of injuries by employers. Web online rate comparisons of all workers' compensation insurers in missouri. Web report your injury immediately. 10/2013) declaration of service i.
Form 110A Download Fillable PDF or Fill Online Employee's Claim for
10/2013) declaration of service i. State of california department of. Failure to report your injury to your employer within 30 days may jeopardize. Please fill out the form completely and accurately. 1 copy for the workers’.
Report Your Injury Immediately To Your Employer Or Supervisor.
Missouri employers involved in the construction. Failure to report your injury to your employer within 30 days may jeopardize. 1 copy for the dia; You will need 3 copies of this form and all other materials:
Record And Report Of Injuries By Employers.
Please fill out the form completely and accurately. Web missouri employers are required to carry workers’ compensation insurance if they have five or more employees. 1 copy for the workers’. You should complete this form when you believe you are not getting all of the.
State Of California Department Of.
Web deu form 110 (rev. Web permanent disability rating determination. You will need 3 copies of this form and all other materials: An employer, or a third party designated by the employer, shall record any injury or illness incurred by one of its employees in the.
10/2013) Declaration Of Service I.
1 copy for the workers’. Notice of options following disability rating (deu form 110). 1 copy for the dia; Web online rate comparisons of all workers' compensation insurers in missouri.