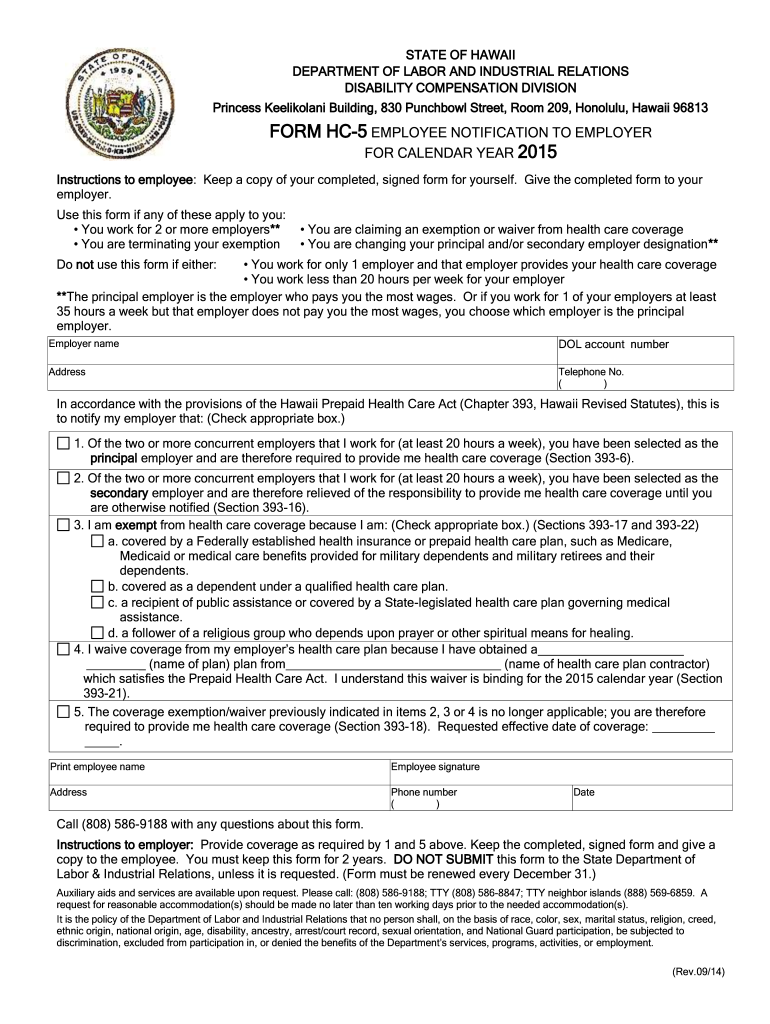
Hc-5 Form
Hc-5 Form - Use this form if the. Web the final due date for your last 2023 estimated tax payment will be january 15th, 2024. To start the form, use the fill camp; One or more applications was installed on the. There shall be allowed as a deduction any loss sustained during the taxable year and not compensated for by. Web low income (you must make your own claim on an hc1 form based on your financial circumstances). • works for 2 or. For glasses and contact lenses, the maximum refund anyone can have is the. Sign online button or tick the preview image of the form. You will need to fill in an hc1 form to apply to the nhs low income.
Employer name dol account number address phone no. You will need to fill in an hc1 form to apply to the nhs low income. Web internal revenue code section 165(h)(5) losses (a) general rule. • works for 2 or. Element name must be a string file: Web the final due date for your last 2023 estimated tax payment will be january 15th, 2024. Works for 2 or more. Web use this form to claim back the cost of a sight test, glasses or contact lenseson low income grounds. Web low income (you must make your own claim on an hc1 form based on your financial circumstances). One or more applications was installed on the.
Web internal revenue code section 165(h)(5) losses (a) general rule. • works for 2 or. Use this form if the employee works at least 20 hours per week and: Web some 46% of americans ages 75 and older and 24% of those ages 65 to 74 report having a disability, according to estimates from the census bureau’s 2021. •works for 2 or more employers** or •claims an exemption or waiver from health care. To start the form, use the fill camp; It is important to make this final payment on time (along with the rest of the payments, of. Use this form if the. Employer name dol account number address phone no. Web the final due date for your last 2023 estimated tax payment will be january 15th, 2024.

HC 510T R Order & Download
There shall be allowed as a deduction any loss sustained during the taxable year and not compensated for by. One or more applications was installed on the. Web low income (you must make your own claim on an hc1 form based on your financial circumstances). Employer name dol account number address phone no. It is important to make this final.
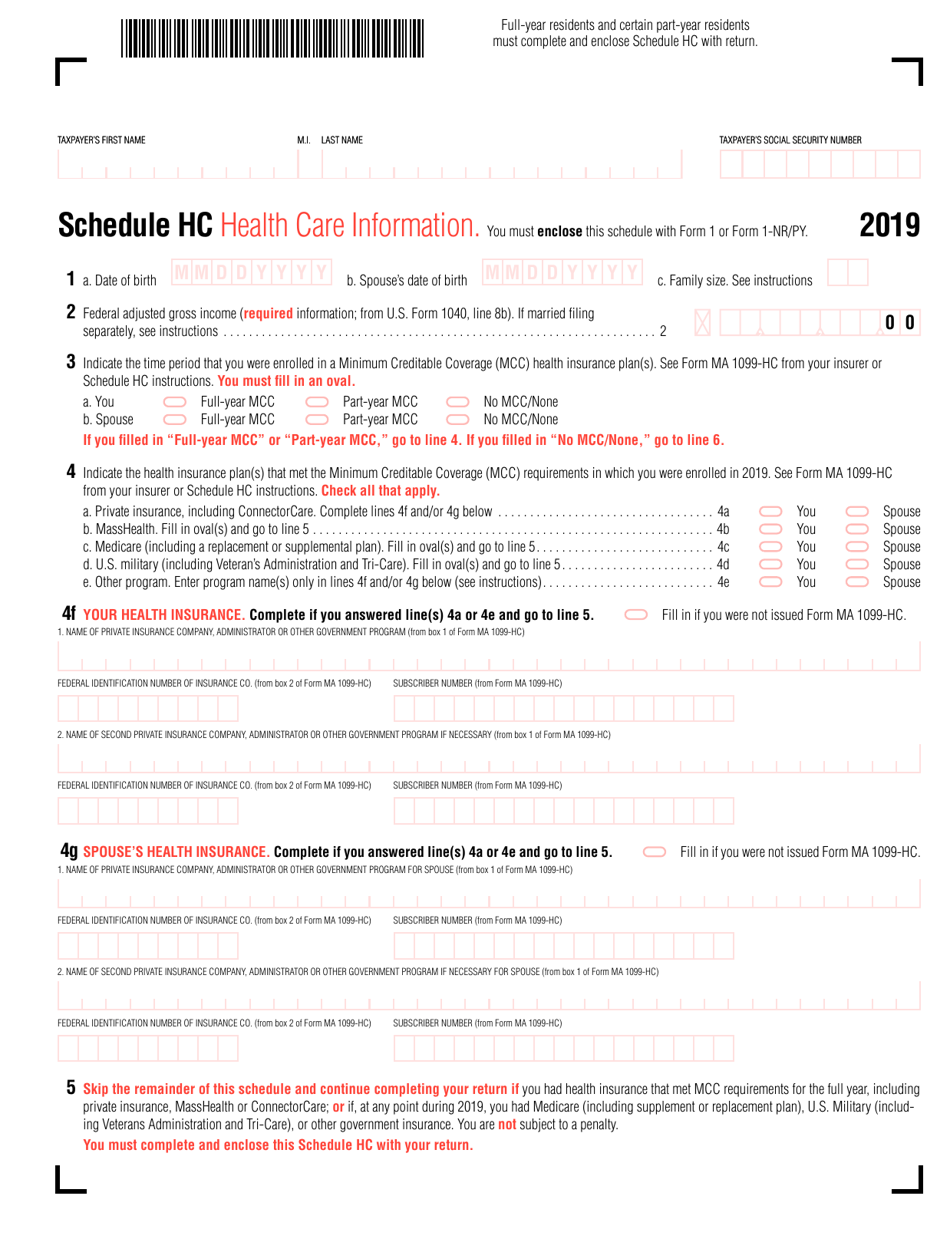
Schedule HC Download Printable PDF or Fill Online Health Care
Sign online button or tick the preview image of the form. Use this form if the. Element name must be a string file: • works for 2 or. Use this form if the.

Hc5 Form Online Fill Online, Printable, Fillable, Blank pdfFiller
Employees must sign this form annually if they waive. • works for 2 or. It is important to make this final payment on time (along with the rest of the payments, of. Use this form if the. Web use this form to claim back the cost of a sight test, glasses or contact lenseson low income grounds.

Autoscript OPTO Desktop Control (USB) HC5 HC5 B&H Photo Video
Sign online button or tick the preview image of the form. Element name must be a string file: Works for 2 or more. There shall be allowed as a deduction any loss sustained during the taxable year and not compensated for by. To start the form, use the fill camp;
HC5 helicopter development history, photos, technical data
Web use this form to claim back the cost of a sight test, glasses or contact lenseson low income grounds. Employees must sign this form annually if they waive. •works for 2 or more employers** or •claims an exemption or waiver from health care. Element name must be a string file: It is important to make this final payment on.

HC 3,5/50mm II
Works for 2 or more. Employer name dol account number address phone no. One or more applications was installed on the. Web internal revenue code section 165(h)(5) losses (a) general rule. It is important to make this final payment on time (along with the rest of the payments, of.

Classifieds ORIGINAL Heil HC5 Element
You will need to fill in an hc1 form to apply to the nhs low income. There shall be allowed as a deduction any loss sustained during the taxable year and not compensated for by. Web internal revenue code section 165(h)(5) losses (a) general rule. Web low income (you must make your own claim on an hc1 form based on.
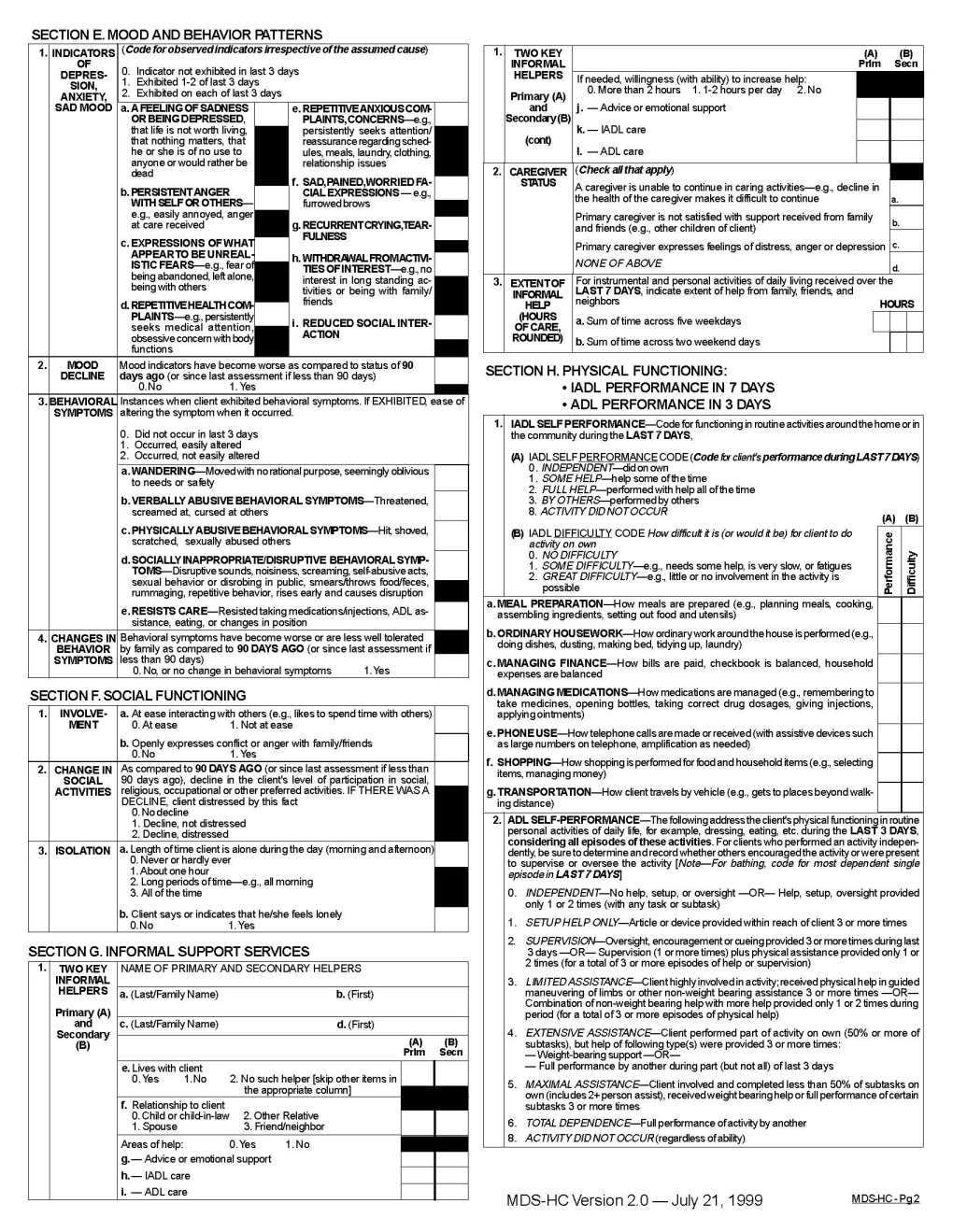
Mds hc 2022 2023 EduVark
Web some 46% of americans ages 75 and older and 24% of those ages 65 to 74 report having a disability, according to estimates from the census bureau’s 2021. Web low income (you must make your own claim on an hc1 form based on your financial circumstances). Works for 2 or more. • works for 2 or. Web use this.

2020 Hc 5 Form Fill Online, Printable, Fillable, Blank pdfFiller
Employer name dol account number address phone no. Element name must be a string file: To start the form, use the fill camp; One or more applications was installed on the. Web some 46% of americans ages 75 and older and 24% of those ages 65 to 74 report having a disability, according to estimates from the census bureau’s 2021.
20152021 Form HI HC5 Fill Online, Printable, Fillable, Blank pdfFiller
To start the form, use the fill camp; Works for 2 or more. Web the final due date for your last 2023 estimated tax payment will be january 15th, 2024. Use this form if the. One or more applications was installed on the.
Web Some 46% Of Americans Ages 75 And Older And 24% Of Those Ages 65 To 74 Report Having A Disability, According To Estimates From The Census Bureau’s 2021.
Web low income (you must make your own claim on an hc1 form based on your financial circumstances). •works for 2 or more employers** or •claims an exemption or waiver from health care. Web the final due date for your last 2023 estimated tax payment will be january 15th, 2024. Use this form if the.
Web Use This Form To Claim Back The Cost Of A Sight Test, Glasses Or Contact Lenseson Low Income Grounds.
Use this form if the. Employees must sign this form annually if they waive. Works for 2 or more. For glasses and contact lenses, the maximum refund anyone can have is the.
Element Name Must Be A String File:
Use this form if the. • works for 2 or. It is important to make this final payment on time (along with the rest of the payments, of. One or more applications was installed on the.
• Works For 2 Or.
You will need to fill in an hc1 form to apply to the nhs low income. There shall be allowed as a deduction any loss sustained during the taxable year and not compensated for by. Employer name dol account number address phone no. Use this form if the employee works at least 20 hours per week and: