Hysterectomy Consent Form For Medicaid
Hysterectomy Consent Form For Medicaid - Web federal regulations (42 cfr 441.255) require that a medicaid recipient undergoing a hysterectomy sign written acknowledgment of receipt of hysterectomy information. Web here, you will find a library of the forms most frequently used by health care professionals. Web information on the state and federal forms required for an abortion, sterilization, or hysterectomy of medicaid beneficiaries are located on the tenncare miscellaneous. Client’s name can be typed or. • enter the name of the representative if the. This form is not available for ordering. Web to submit a sterilization consent form. Use the tools and resources. Get the tools you need to easily manage your administrative needs, and your keep your focus on the health of your patients. Web a copy of the mco id card, which covers the date of the hysterectomy, or a copy of the retroactive approval notice, must accompany this form before reimbursement can be.
Web nc medicaid reproductive health forms including abortion, hysterectomy, pregnancy medical home, pregnancy risk screening and sterilization. • enter the diagnosis code. Looking for a form but don’t see it here? Health benefits/nc medicaid (dhb) form effective date. Member name member id provider name npi/provider number part a. Beginning april 1, 2023, the family support division will be required to restart annual renewals for mo healthnet. Web ☐ abortion consent form ☐ hysterectomy consent form ☐ medical records ☐ corrected claim ☐ invoice ☐ other health insurance information ☐ er level of payment. Claims submitted with any of. Describe the nature of the emergency: Web to submit a sterilization consent form.
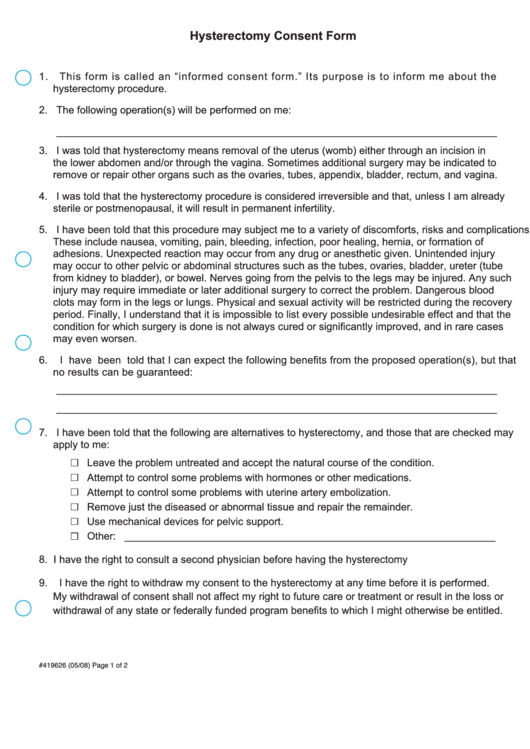
This form is not available for ordering. Web nc medicaid reproductive health forms including abortion, hysterectomy, pregnancy medical home, pregnancy risk screening and sterilization. This form is not available. Health benefits/nc medicaid (dhb) form effective date. Client’s name can be typed or. • enter the name of the representative if the. Please contact your provider representative for. Web a copy of the mco id card, which covers the date of the hysterectomy, or a copy of the retroactive approval notice, must accompany this form before reimbursement can be. Member name member id provider name npi/provider number part a. Web this is the hysterectomy consent form that acknowledges the patient's receipt of hysterectomy information.

Ohio Medicaid Sterilization Consent Form 2022 Printable Consent Form 2022
Client’s name can be typed or. Web federal regulations (42 cfr 441.255) require that a medicaid recipient undergoing a hysterectomy sign written acknowledgment of receipt of hysterectomy information. Use the tools and resources. This form is not available for ordering. Web to submit a sterilization consent form.

Ohio Medicaid Hysterectomy Consent Form 2022 Printable Consent Form 2022
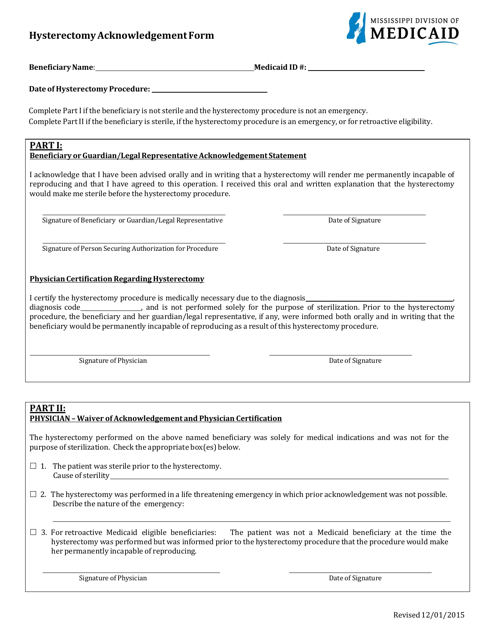
Web a copy of the mco id card, which covers the date of the hysterectomy, or a copy of the retroactive approval notice, must accompany this form before reimbursement can be. Web hysterectomy acknowledgment of consent form. The hysterectomy was performed in a life threatening emergency in which prior acknowledgement was not possible. Use the tools and resources. Web •.
Top 7 Hysterectomy Consent Form Templates free to download in PDF format
Looking for a form but don’t see it here? Web instructions for completing the hysterectomy acknowledgment form always complete this section 1. Web to submit a sterilization consent form. Web here, you will find a library of the forms most frequently used by health care professionals. Consent form required a hysterectomy informed consent form is required for claims submitted for.
Mississippi Hysterectomy Acknowledgement Form Download Fillable PDF
Claims submitted with any of. Client’s name can be typed or. Please contact your provider representative for. • enter the diagnosis code. Web (nys medicaid program) either part i or part ii must be completed recipient id no.
Hysterectomy Cancer Side Effects Lawsuit
• enter the name of the representative if the. Web federal regulations (42 cfr 441.255) require that a medicaid recipient undergoing a hysterectomy sign written acknowledgment of receipt of hysterectomy information. Client’s name can be typed or. The hysterectomy was performed in a life threatening emergency in which prior acknowledgement was not possible. • enter the diagnosis code.
Top 12 Patient Acknowledgement Form Templates free to download in PDF
This form is not available for ordering. Web (nys medicaid program) either part i or part ii must be completed recipient id no. Client’s name can be typed or. Web this is the hysterectomy consent form that acknowledges the patient's receipt of hysterectomy information. Claims submitted with any of.
PPT DEPARTMENT OF PUBLIC HEALTH AND HUMAN SERVICES HEALTH RESOURCES
Web this is the hysterectomy consent form that acknowledges the patient's receipt of hysterectomy information. • enter the diagnosis code. Web (nys medicaid program) either part i or part ii must be completed recipient id no. Please contact your provider representative for. Get the tools you need to easily manage your administrative needs, and your keep your focus on the.

Medicaid Hysterectomy Consent Form Consent Form
• enter the diagnosis description requiring hysterectomy. Web information on the state and federal forms required for an abortion, sterilization, or hysterectomy of medicaid beneficiaries are located on the tenncare miscellaneous. Describe the nature of the emergency: • enter the name of the representative if the. Web hysterectomy consent, english & spanish *see below.

Hysterectomy Consent Form For Ohio Medicaid 2023 Printable Consent
Web (nys medicaid program) either part i or part ii must be completed recipient id no. This form is not available. Web a copy of the mco id card, which covers the date of the hysterectomy, or a copy of the retroactive approval notice, must accompany this form before reimbursement can be. Web this is the hysterectomy consent form that.
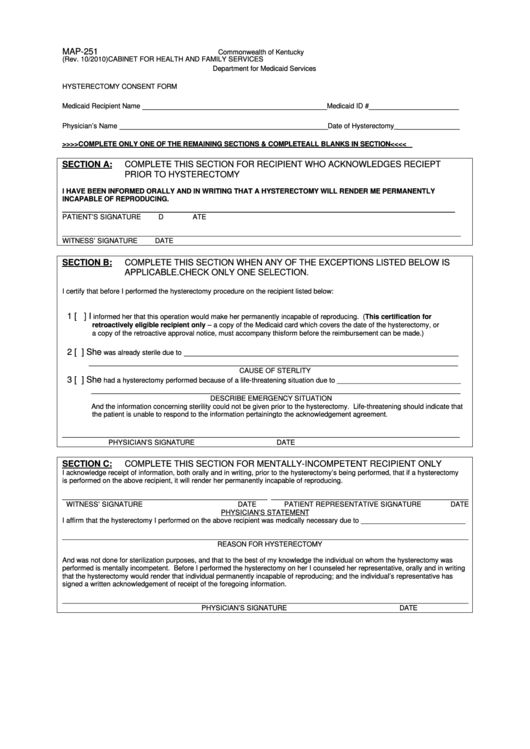
Form Map251 Hysterectomy Consent Form printable pdf download
Web federal regulations (42 cfr 441.255) require that a medicaid recipient undergoing a hysterectomy sign written acknowledgment of receipt of hysterectomy information. Web hysterectomy acknowledgment of consent form. Use the tools and resources. Web this is the hysterectomy consent form that acknowledges the patient's receipt of hysterectomy information. The hysterectomy was performed in a life threatening emergency in which prior.
Web This Is The Hysterectomy Consent Form That Acknowledges The Patient's Receipt Of Hysterectomy Information.
Health benefits/nc medicaid (dhb) form effective date. Web federal regulations (42 cfr 441.255) require that a medicaid recipient undergoing a hysterectomy sign written acknowledgment of receipt of hysterectomy information. Web here, you will find a library of the forms most frequently used by health care professionals. • enter the name of the representative if the.
• Enter The Diagnosis Code.
Web payment by louisiana’s medicaid program cannot be authorized for any hysterectomy performed solely for the purpose of rendering an individual permanently incapable of. Web ☐ abortion consent form ☐ hysterectomy consent form ☐ medical records ☐ corrected claim ☐ invoice ☐ other health insurance information ☐ er level of payment. Web nc medicaid reproductive health forms including abortion, hysterectomy, pregnancy medical home, pregnancy risk screening and sterilization. Consent form required a hysterectomy informed consent form is required for claims submitted for hysterectomy services.
1 Patient Information [19] [9] Patient Name (Print First And Last Name) Patient Date Of Birth (Mm/Dd/Yyyy) [25][4] Apple Health Client Id.
Web hysterectomy acknowledgment of consent form. Looking for a form but don’t see it here? Web hysterectomy consent, english & spanish *see below. Please contact your provider representative for.
This Form Is Not Available.
Member name member id provider name npi/provider number part a. The hysterectomy was performed in a life threatening emergency in which prior acknowledgement was not possible. Web • enter the recipient’s 13 digit medicaid number. Web (nys medicaid program) either part i or part ii must be completed recipient id no.