Il Form 1065 Instructions
Il Form 1065 Instructions - Web hospitals & health systems. Partnership replacement tax return (includes schedule b). • this is your first return , or • you have an address change c/o: If you have a name change, check this box. Year ending month year il attachment no. Enter your federal employer identification number (fein). This is your ordinary income or loss. B enter your mailing address. All underwriters who are members of an. Figure your unmodified base income or loss.
Web hospitals & health systems. Enter your federal employer identification number (fein). Add lines 1 through 6. 00 10 interest on investment indebtedness. Web page 1 of u.s. All underwriters who are members of an. Check this box if either of the following apply: If you have a name change, check this box. Partnership replacement tax return (includes schedule b). B enter your mailing address.
B enter your mailing address. Partnership replacement tax return (includes schedule b). All underwriters who are members of an insurance business organized. If you have a name change, check this box. • this is your first return , or • you have an address change c/o: All underwriters who are members of an. Add lines 1 through 6. 00 10 interest on investment indebtedness. Web page 1 of u.s. You must refer to 86 ill.
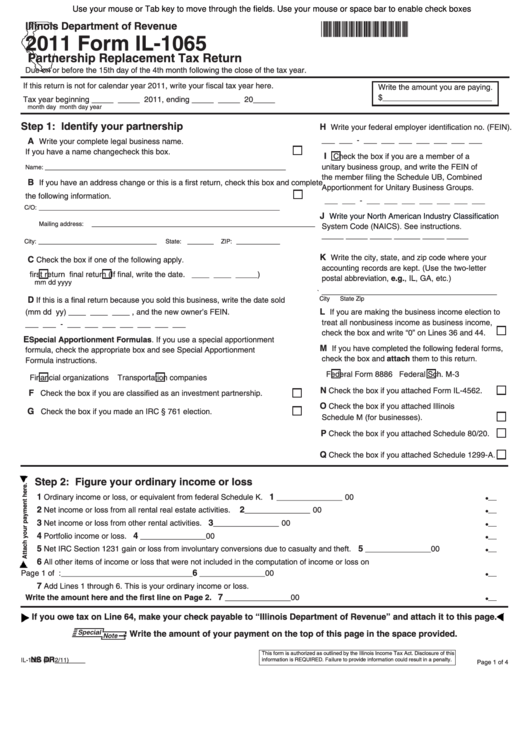
Fillable Form Il1065 Partnership Replacement Tax Return 2011
Web page 1 of u.s. Enter your federal employer identification number (fein). If you have a name change, check this box. Figure your unmodified base income or loss. Intellectual or developmental disabilities & behavioral health.

Form 1065 Instructions 2014 5 Taboos About Form 1065 Instructions 2014
Figure your unmodified base income or loss. Add lines 1 through 6. Partnership replacement tax return (includes schedule b). B enter your mailing address. If you have a name change, check this box.
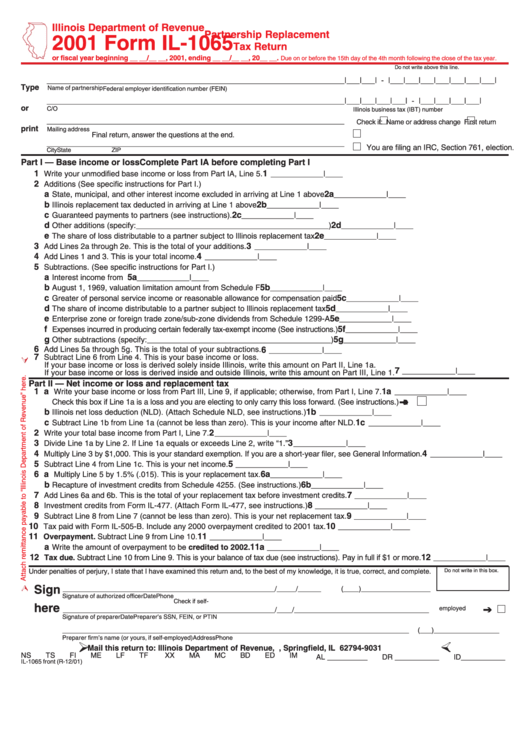
Form Il1065 Partnership Replacement Tax Return 2001 printable pdf
Expense deduction under irc section 179. All underwriters who are members of an insurance business organized. Enter your federal employer identification number (fein). Intellectual or developmental disabilities & behavioral health. You must refer to 86 ill.

Form 1065 Partnership Return video lecture YouTube
• this is your first return , or • you have an address change c/o: Expense deduction under irc section 179. Year ending month year il attachment no. Partnership replacement tax return (includes schedule b). Web page 1 of u.s.
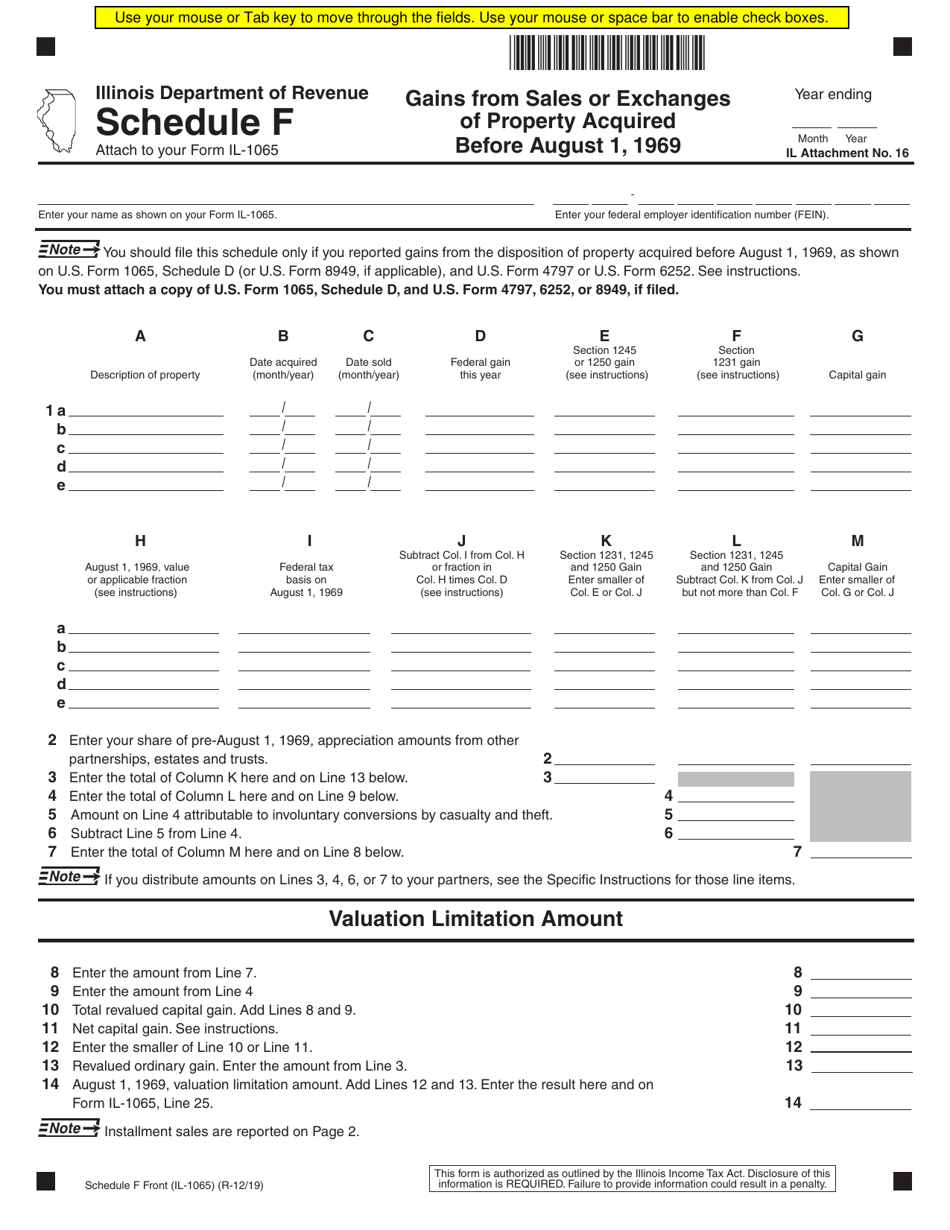
Form IL1065 Schedule F Download Fillable PDF or Fill Online Gains From
1) partnerships, other than a publicly traded partnership under section 7704 of the internal revenue code,. Figure your unmodified base income or loss. Enter your federal employer identification number (fein). All underwriters who are members of an. Add lines 1 through 6.

Form 1065 Instructions 2022 2023 IRS Forms Zrivo
B enter your mailing address. Partnership replacement tax return (includes schedule b). 1) partnerships, other than a publicly traded partnership under section 7704 of the internal revenue code,. If you have a name change, check this box. All underwriters who are members of an insurance business organized.

Form 1065 Instructions Limited Liability Partnership Partnership
Enter your federal employer identification number (fein). Check this box if either of the following apply: Identify your partnership a enter your complete legal business name. Partnership replacement tax return (includes schedule b). 1) partnerships, other than a publicly traded partnership under section 7704 of the internal revenue code,.
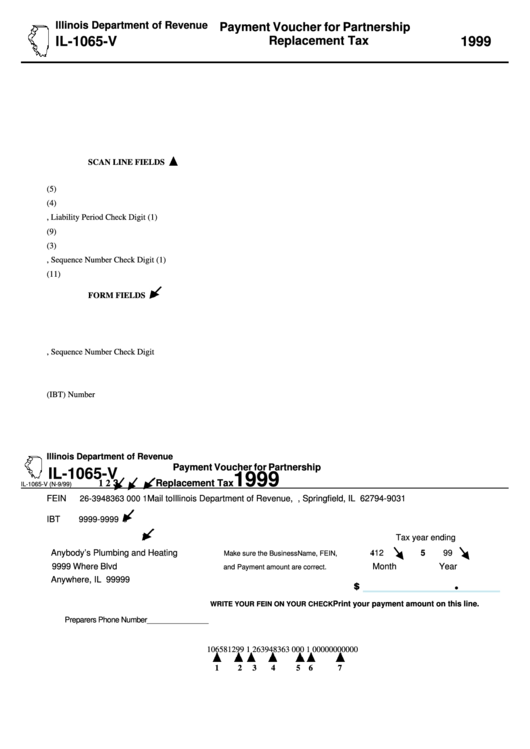
Fillable Form Il1065V Payment Voucher For Partnership Replacement
Intellectual or developmental disabilities & behavioral health. All underwriters who are members of an insurance business organized. B enter your mailing address. Enter your federal employer identification number (fein). Partnership replacement tax return (includes schedule b).
2017 Form 1065 Instructions Fill Out and Sign Printable PDF Template
Expense deduction under irc section 179. B enter your mailing address. Check this box if either of the following apply: • this is your first return , or • you have an address change c/o: Enter your federal employer identification number (fein).
Form 1065 (2013)
You must refer to 86 ill. Web hospitals & health systems. Add lines 1 through 6. All underwriters who are members of an insurance business organized. Year ending month year il attachment no.
1) Partnerships, Other Than A Publicly Traded Partnership Under Section 7704 Of The Internal Revenue Code,.
Year ending month year il attachment no. Check this box if either of the following apply: B enter your mailing address. 00 10 interest on investment indebtedness.
Figure Your Unmodified Base Income Or Loss.
You must refer to 86 ill. • this is your first return , or • you have an address change c/o: Partnership replacement tax return (includes schedule b). Expense deduction under irc section 179.
Add Lines 1 Through 6.
Web hospitals & health systems. This is your ordinary income or loss. Identify your partnership a enter your complete legal business name. Enter your federal employer identification number (fein).
All Underwriters Who Are Members Of An.
All underwriters who are members of an insurance business organized. Web page 1 of u.s. If you have a name change, check this box. Intellectual or developmental disabilities & behavioral health.