Medimpact Dmr Form
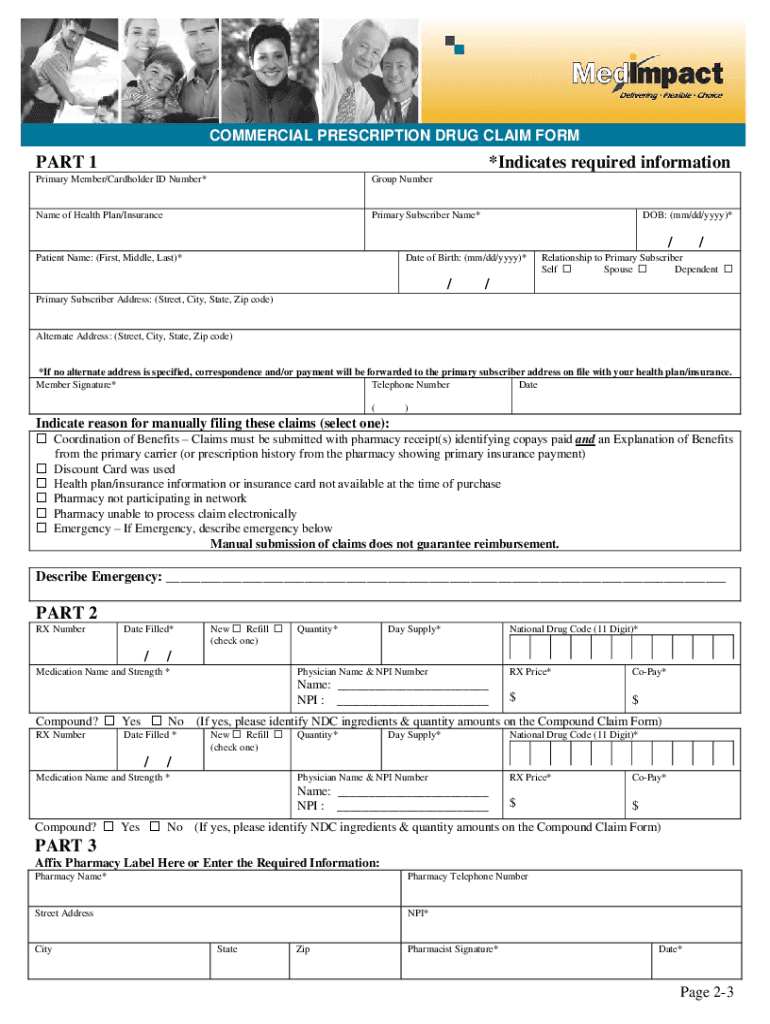
Medimpact Dmr Form - Web at medimpact, we’re committed to making it even easier for members to manage their medications and related costs. Learn more about my benefits. The member/cardholder id number is located on your insurance card. Complete all information under part 1. Some pharmacy chains are not set up yet for direct coverage using insurance; Illinois medicaid state pa form. Medimpact is an independent partner, free from ownership interests with health plans and pharmacy chains that. Form is true and correct to the best of my knowledge. Web presenting your medimpact id card will enable you to receive kits at no cost. We are informing and empowering millions of americans to lead healthier lives.
Web we offer clients peace of mind knowing that their pbm is perfectly aligned with their goals and fully invested in their future. Web medimpact claim form we use cookies to make interactions with our website easy and meaningful. Some pharmacy chains are not set up yet for direct coverage using insurance; Web the medication request form (mrf) is submitted by participating physicians and providers to obtain coverage for formulary drugs requiring prior authorization (pa); Web welcome finally, pharmacy benefits that benefit you. Web presenting your medimpact id card will enable you to receive kits at no cost. And overrides of pharmacy management procedures such as step therapy, quantity limit, or other edits. Arrange for home delivery or find a pharmacy with the lowest price? Member or authorized representative signature* date* That's why we have a team of experts and a variety of help resources to make requests faster and easier.
Pharmacist’s signature required when bottom portion of claim form is completed by pharmacy or dispensing facility only. What is the cost for the direct member reimbursement (dmr) paper processing? Web we offer clients peace of mind knowing that their pbm is perfectly aligned with their goals and fully invested in their future. The dmr form is to be submitted directly to medimpact for reimbursement of pharmacy costs. Arrange for home delivery or find a pharmacy with the lowest price? If you purchase a kit and pay at the register, use the medimpact covid home test kit dmr form to receive reimbursement. By continuing to use this site, you are giving us your consent. And overrides of pharmacy management procedures such as step therapy, quantity limit or other edits. Submit claims within the filing period specified by your health plan. Web as long as medimpact is delegated to process direct member reimbursement (dmr) on your behalf, the member may submit a dmr form to medimpact to determine if the claim is eligible for reimbursement.
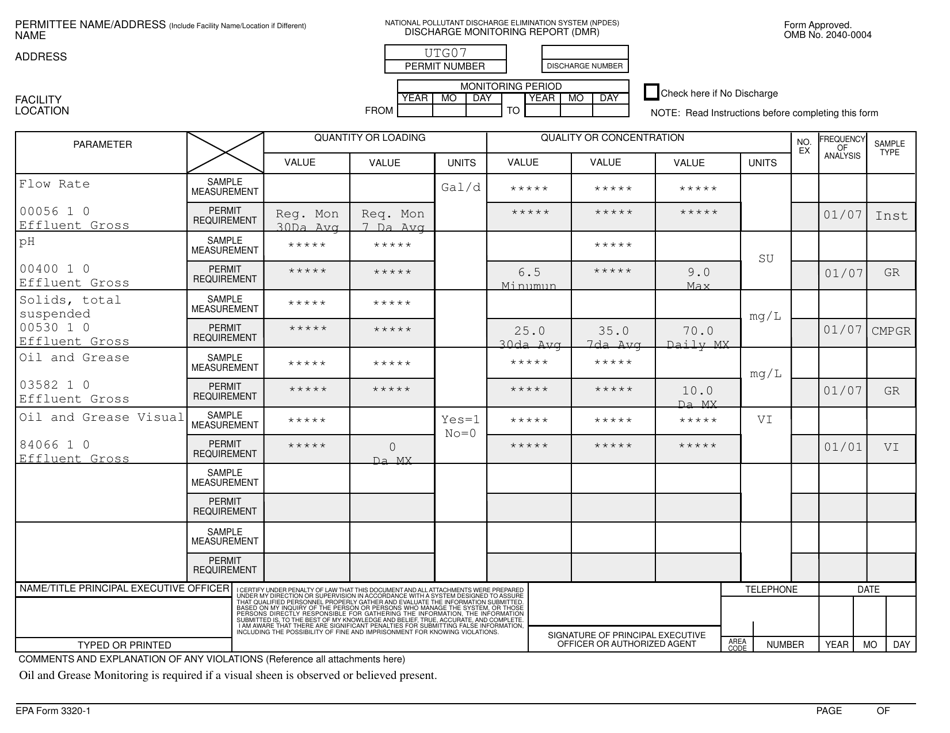
EPA Form 33201 Fill Out, Sign Online and Download Fillable PDF
Web the medication request form (mrf) is submitted by participating physicians and providers to obtain coverage for formulary drugs requiring prior authorization (pa); We are informing and empowering millions of americans to lead healthier lives. What is the cost for the direct member reimbursement (dmr) paper processing? Member or authorized representative signature* date* Send the completed form and receipt(s) to:
Fillable Epa Form 33201 (Rev. 399) Discharge Monitoring Report (Dmr
Web presenting your medimpact id card will enable you to receive kits at no cost. Learn more about my benefits. Web at medimpact, we’re committed to making it even easier for members to manage their medications and related costs. Web medimpact claim form we use cookies to make interactions with our website easy and meaningful. X page 2 revision 01.30.19.

For clients. MedImpact
Web the medication request form (mrf) is submitted by participating physicians and providers to obtain coverage for formulary drugs requiring prior authorization (pa); The dmr form is to be submitted directly to medimpact for reimbursement of pharmacy costs. By filling out and delivering a prior authorization form, the. Indiana state medicaid pa form. And overrides of pharmacy management procedures such.
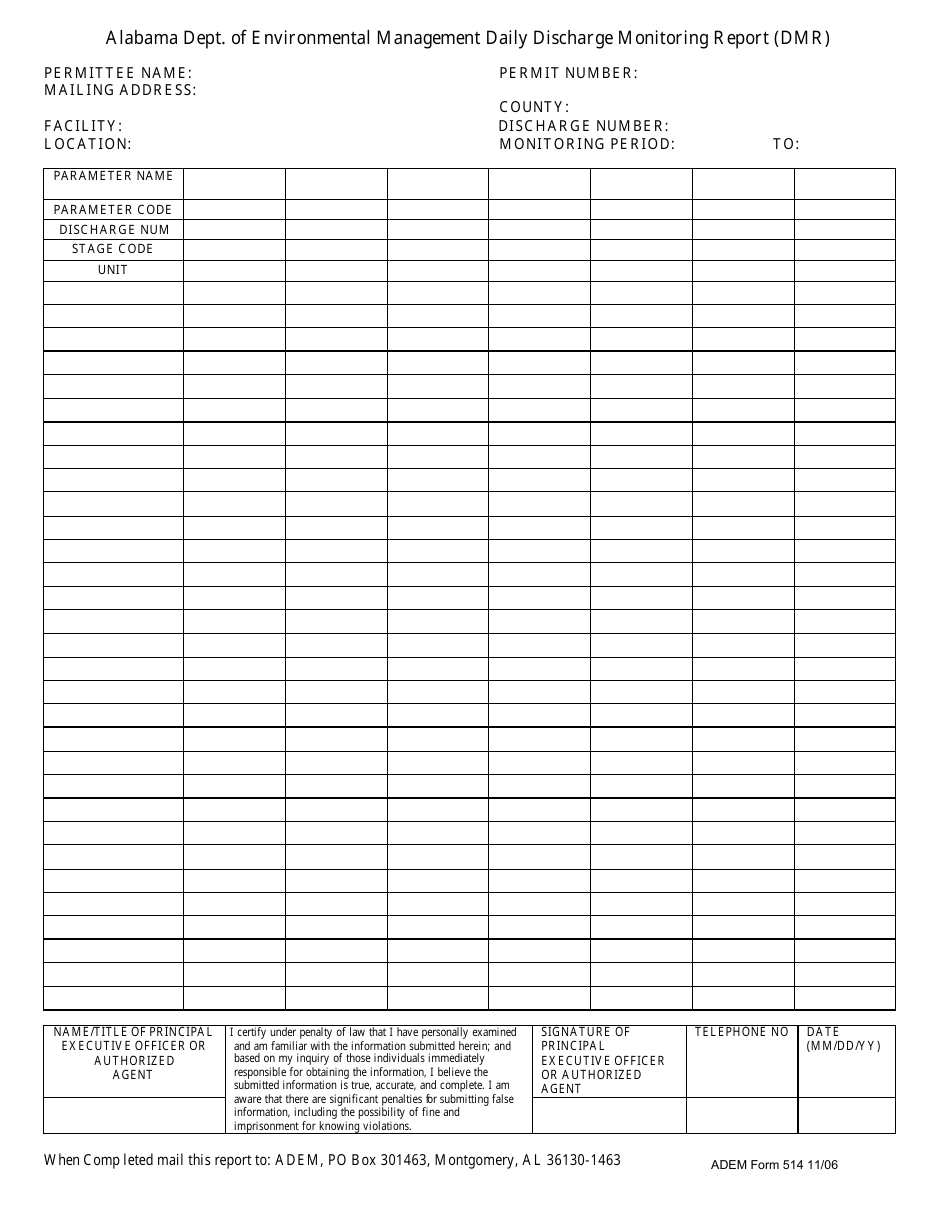
ADEM Form 514 Download Fillable PDF or Fill Online Daily Discharge
And overrides of pharmacy management procedures such as step therapy, quantity limit or other edits. Indiana state medicaid pa form. For questions about your filing period, please call the number on. Web medimpact direct member reimbursement. Web you can call medimpact direct® to update this information at any time or you can update your payment preferences by signing in to.

20132021 Form OPTUMRx 1040006 Fill Online, Printable, Fillable, Blank
Web 2019 10181 scripps gateway court san diego, ca 92131 fax: Web at medimpact, we’re committed to making it even easier for members to manage their medications and related costs. Indiana state medicaid pa form. Web medimpact direct member reimbursement. X page 2 revision 01.30.19 mail this completed order form, with your prescription and payment information, to:
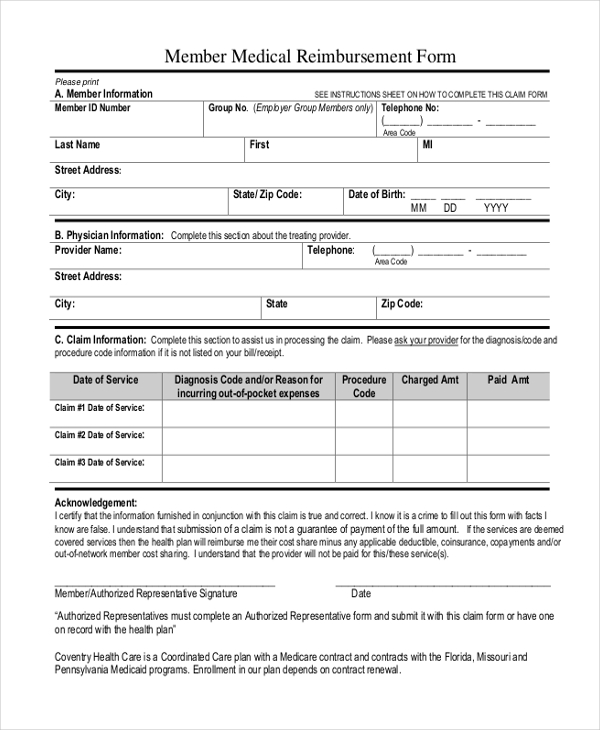
FREE 9+ Sample Medicaid Reimbursement Forms in MS Word PDF
Indiana state medicaid pa form. X page 2 revision 01.30.19 mail this completed order form, with your prescription and payment information, to: Web the medication request form is submitted by participating physicians and providers to obtain coverage for formulary drugs requiring prior authorization (pa); And overrides of pharmacy management procedures such as step therapy, quantity limit or other edits. Web.

2014 OPTUMRx Nuvigil & Provigil Prior Authorization Request Form Fill
What is the cost for the direct member reimbursement (dmr) paper processing? The dmr form is to be submitted directly to medimpact for reimbursement of pharmacy costs. Indiana state medicaid pa form. Web 2019 10181 scripps gateway court san diego, ca 92131 fax: Web presenting your medimpact id card will enable you to receive kits at no cost.
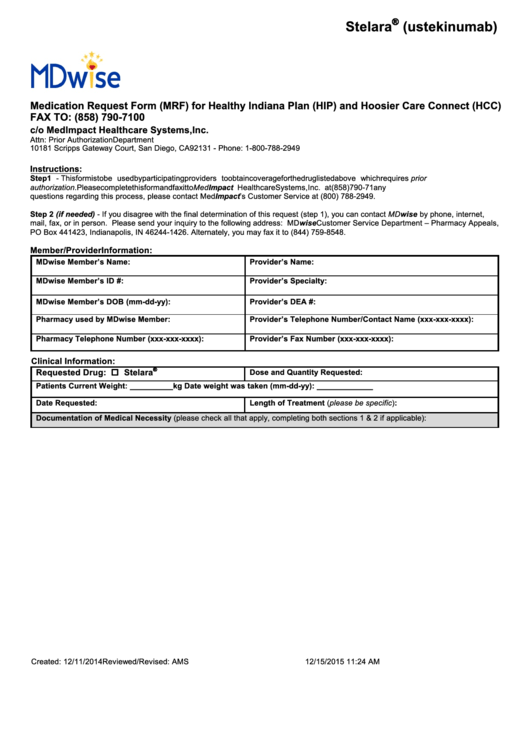
Fillable Mdwise Medication Request Form (Mrf) For Healthy Indiana Plan
By filling out and delivering a prior authorization form, the. Member or authorized representative signature* date* Web as long as medimpact is delegated to process direct member reimbursement (dmr) on your behalf, the member may submit a dmr form to medimpact to determine if the claim is eligible for reimbursement. What is the cost for the direct member reimbursement (dmr).
Medimpact Reimbursement Form Fill Out and Sign Printable PDF Template
That's why we have a team of experts and a variety of help resources to make requests faster and easier. Web the medication request form (mrf) is submitted by participating physicians and providers to obtain coverage for formulary drugs requiring prior authorization (pa); Web 2019 10181 scripps gateway court san diego, ca 92131 fax: We know pa requests are complex..
Missouri Discharge Fill Online, Printable, Fillable, Blank pdfFiller
Pharmacist’s signature required when bottom portion of claim form is completed by pharmacy or dispensing facility only. Member or authorized representative signature* date* Form is true and correct to the best of my knowledge. By continuing to use this site, you are giving us your consent. Web the medication request form is submitted by participating physicians and providers to obtain.
Illinois Medicaid State Pa Form.
Web as long as medimpact is delegated to process direct member reimbursement (dmr) on your behalf, the member may submit a dmr form to medimpact to determine if the claim is eligible for reimbursement. Medimpact is an independent partner, free from ownership interests with health plans and pharmacy chains that. Web the medication request form (mrf) is submitted by participating physicians and providers to obtain coverage for formulary drugs requiring prior authorization (pa); For questions about your filing period, please call the number on.
That's Why We Have A Team Of Experts And A Variety Of Help Resources To Make Requests Faster And Easier.
Web medimpact claim form we use cookies to make interactions with our website easy and meaningful. The member/cardholder id number is located on your insurance card. Pharmacist’s signature required when bottom portion of claim form is completed by pharmacy or dispensing facility only. Need to access and understand your prescription benefits?
And Overrides Of Pharmacy Management Procedures Such As Step Therapy, Quantity Limit Or Other Edits.
Learn how cookies are used on our site. Submit claims within the filing period specified by your health plan. Web welcome finally, pharmacy benefits that benefit you. The dmr form is to be submitted directly to medimpact for reimbursement of pharmacy costs.
X Page 2 Revision 01.30.19 Mail This Completed Order Form, With Your Prescription And Payment Information, To:
And overrides of pharmacy management procedures such as step therapy, quantity limit, or other edits. Web medimpact direct member reimbursement. Web presenting your medimpact id card will enable you to receive kits at no cost. Indiana state medicaid pa form.