Sleep Study Referral Form
Sleep Study Referral Form - Send referral by fax or email to the following address: Sleepstudy@airliquide.com alh will contact you within 5 working days to book your sleep study stamp. Yes no • if yes, please provide the date of the last sleep study: Medical personnel associated with lifespan you may place a referral via lifechart. Web our sleep navigators will review your patient’s history and determine appropriate next steps for consultation and sleep testing. If you need sleep services, please have your primary care physician contact our referral service to schedule an appointment: Web details of the sleep history, physical exam and reason for referral. Web to refer a patient for a sleep study, complete the referral form and fax to the appropriate sleep lab location. We will arrange for appropriate diagnostic and therapeutic procedures. This completed form medical records related to the chief complaint
Sleepstudy@airliquide.com alh will contact you within 5 working days to book your sleep study stamp. Web step 1 make sure that referral has been fully completed. Web to refer a patient for a sleep study, complete the referral form and fax to the appropriate sleep lab location. (check all that apply) loud snoring cyanosis/hypoxia on cpap/bipap bedtime resistance restless legs symptoms choking/gasping arousals alte daytime sleepiness difficulty falling asleep sleepwalking. Send referral by fax or email to the following address: Adult patients pediatric patients form sleep lab referral form information packets sleep lab overnight study info packet home sleep study info packet Yes no • if yes, please provide the date of the last sleep study: This completed form medical records related to the chief complaint Web download and print a sleep study prescription referral form, and take it to your primary care physician to complete. We will arrange for appropriate diagnostic and therapeutic procedures.
Web step 1 make sure that referral has been fully completed. Web a referral is needed to place an order for a sleep study test. Send referral by fax or email to the following address: Web to refer a patient for a sleep study, complete the referral form and fax to the appropriate sleep lab location. Yes no • if yes, please provide the date of the last sleep study: We will arrange for appropriate diagnostic and therapeutic procedures. Web details of the sleep history, physical exam and reason for referral. Booking an appointment (use contact details below) on the day of your test This completed form medical records related to the chief complaint Adult patients pediatric patients form sleep lab referral form information packets sleep lab overnight study info packet home sleep study info packet

News Pediatric Neurology Epilepsy Sleep Medicine Brain Injury
You must have your physician's signature in order to schedule an appointment. Sleepstudy@airliquide.com alh will contact you within 5 working days to book your sleep study stamp. This completed form medical records related to the chief complaint Yes no • if yes, please provide the date of the last sleep study: Adult patients pediatric patients form sleep lab referral form.

Weymouth sleep centre referral form
If you need sleep services, please have your primary care physician contact our referral service to schedule an appointment: Send referral by fax or email to the following address: Web download and print a sleep study prescription referral form, and take it to your primary care physician to complete. We will arrange for appropriate diagnostic and therapeutic procedures. (check all.

Sleep Study Requisition Form Sleep Disorders Referral Form Cloud Practice
(check all that apply) loud snoring cyanosis/hypoxia on cpap/bipap bedtime resistance restless legs symptoms choking/gasping arousals alte daytime sleepiness difficulty falling asleep sleepwalking. Sleepstudy@airliquide.com alh will contact you within 5 working days to book your sleep study stamp. Web learn about the expertise and wide range of services — including overnight sleep studies — offered for people with rare and.

Sleep Disorder Referral Form Toronto Sleep Institute Juno EMR
Order the sleep study as an internal referral to “ambulatory referral for sleep studies” or use ref99 by doing the following: We will arrange for appropriate diagnostic and therapeutic procedures. Booking an appointment (use contact details below) on the day of your test Web a referral is needed to place an order for a sleep study test. Web step 1.
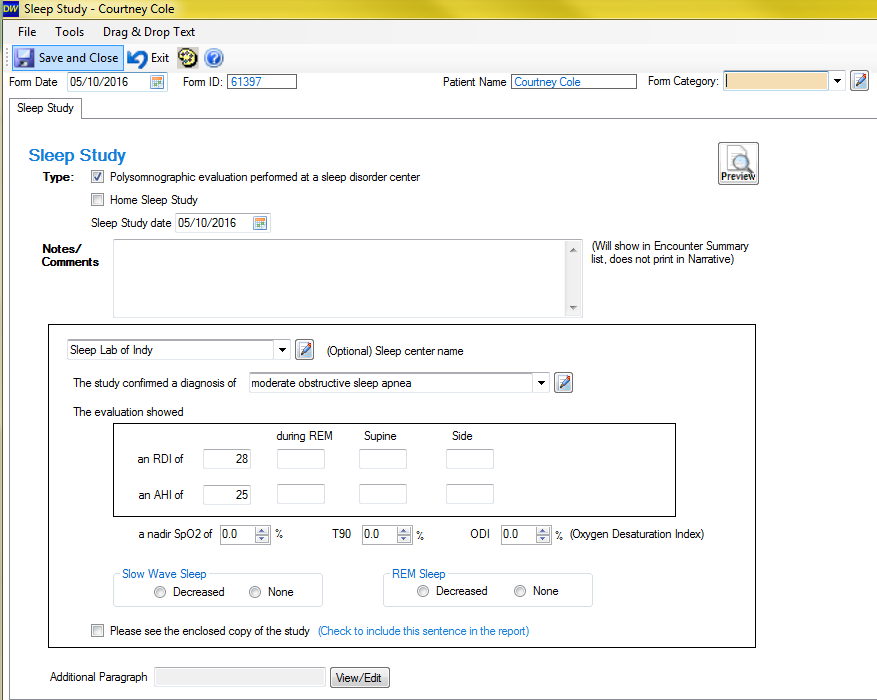
Adding or editing a sleep study in a patient chart
Adult patients pediatric patients form sleep lab referral form information packets sleep lab overnight study info packet home sleep study info packet Web details of the sleep history, physical exam and reason for referral. (check all that apply) loud snoring cyanosis/hypoxia on cpap/bipap bedtime resistance restless legs symptoms choking/gasping arousals alte daytime sleepiness difficulty falling asleep sleepwalking. Sleepstudy@airliquide.com alh will.
Sleep Medical Center SCOFA Find Sleep Medicine Professionals & Services
Web step 1 make sure that referral has been fully completed. Web a referral is needed to place an order for a sleep study test. Yes no • if yes, please provide the date of the last sleep study: Send referral by fax or email to the following address: We will arrange for appropriate diagnostic and therapeutic procedures.
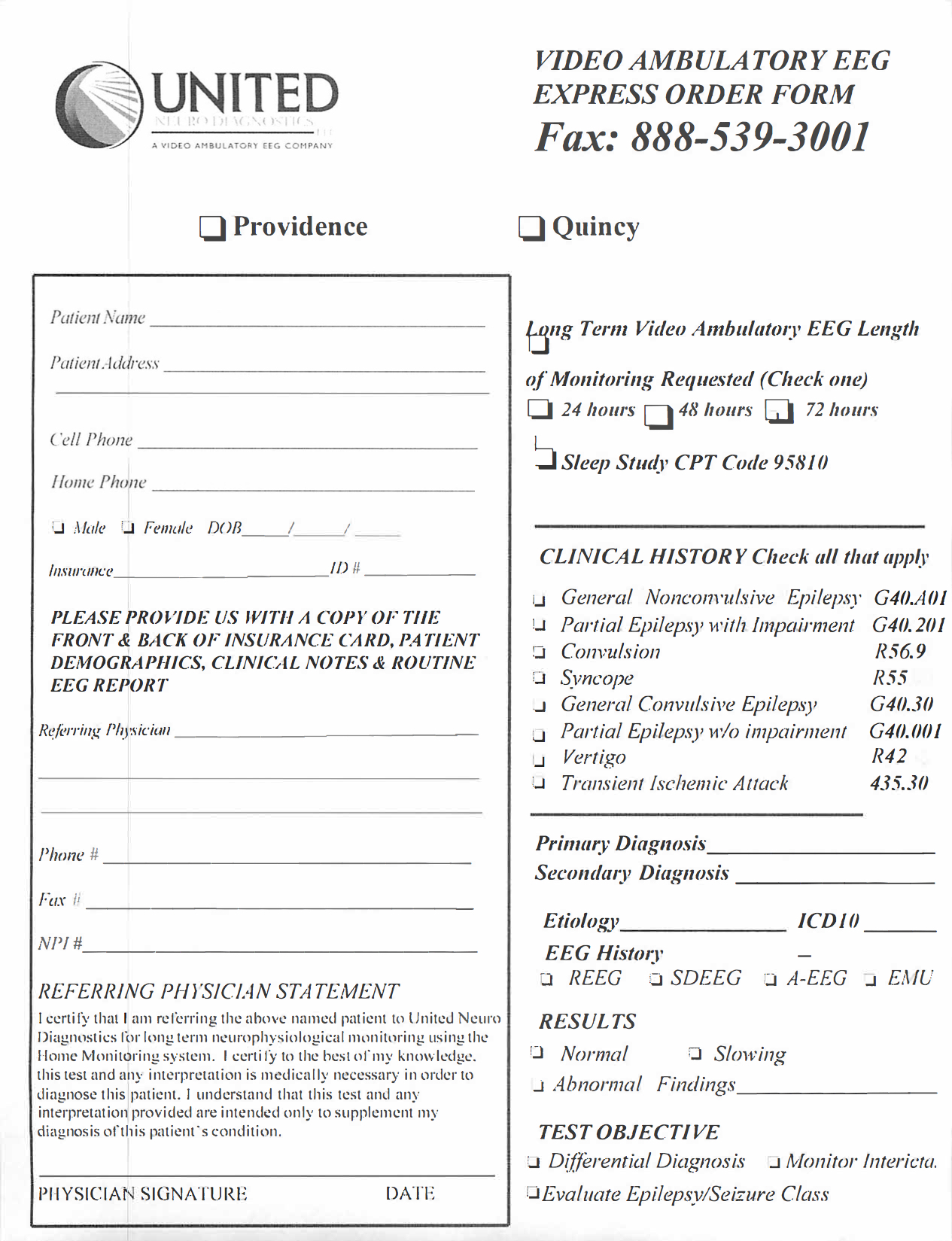
Forms United Sleep Diagnostics
Sleepstudy@airliquide.com alh will contact you within 5 working days to book your sleep study stamp. Medical personnel associated with lifespan you may place a referral via lifechart. We will arrange for appropriate diagnostic and therapeutic procedures. Web a referral is needed to place an order for a sleep study test. Web details of the sleep history, physical exam and reason.

4933E MedSleep Sleep Disorder Referral Form Fredericton Intrahealth
Sleepstudy@airliquide.com alh will contact you within 5 working days to book your sleep study stamp. (check all that apply) loud snoring cyanosis/hypoxia on cpap/bipap bedtime resistance restless legs symptoms choking/gasping arousals alte daytime sleepiness difficulty falling asleep sleepwalking. Web learn about the expertise and wide range of services — including overnight sleep studies — offered for people with rare and.
FREE 7+ Medical Referral Forms in PDF MS Word
(check all that apply) loud snoring cyanosis/hypoxia on cpap/bipap bedtime resistance restless legs symptoms choking/gasping arousals alte daytime sleepiness difficulty falling asleep sleepwalking. Web step 1 make sure that referral has been fully completed. Send referral by fax or email to the following address: Web to refer a patient for a sleep study, complete the referral form and fax to.

News Pediatric Neurology Epilepsy Sleep Medicine Brain Injury
Order the sleep study as an internal referral to “ambulatory referral for sleep studies” or use ref99 by doing the following: Web learn about the expertise and wide range of services — including overnight sleep studies — offered for people with rare and common sleep disorders. Web our sleep navigators will review your patient’s history and determine appropriate next steps.
Web Step 1 Make Sure That Referral Has Been Fully Completed.
Web download and print a sleep study prescription referral form, and take it to your primary care physician to complete. This completed form medical records related to the chief complaint Medical personnel associated with lifespan you may place a referral via lifechart. Adult patients pediatric patients form sleep lab referral form information packets sleep lab overnight study info packet home sleep study info packet
Booking An Appointment (Use Contact Details Below) On The Day Of Your Test
We will arrange for appropriate diagnostic and therapeutic procedures. If you need sleep services, please have your primary care physician contact our referral service to schedule an appointment: Web to refer a patient for a sleep study, complete the referral form and fax to the appropriate sleep lab location. (check all that apply) loud snoring cyanosis/hypoxia on cpap/bipap bedtime resistance restless legs symptoms choking/gasping arousals alte daytime sleepiness difficulty falling asleep sleepwalking.
Send Referral By Fax Or Email To The Following Address:
Web a referral is needed to place an order for a sleep study test. Web details of the sleep history, physical exam and reason for referral. You must have your physician's signature in order to schedule an appointment. Order the sleep study as an internal referral to “ambulatory referral for sleep studies” or use ref99 by doing the following:
Web Learn About The Expertise And Wide Range Of Services — Including Overnight Sleep Studies — Offered For People With Rare And Common Sleep Disorders.
Yes no • if yes, please provide the date of the last sleep study: Web our sleep navigators will review your patient’s history and determine appropriate next steps for consultation and sleep testing. Sleepstudy@airliquide.com alh will contact you within 5 working days to book your sleep study stamp.