Wheelchair Evaluation Form
Wheelchair Evaluation Form - We must identify the primary as well as all potentially relevant secondary diagnoses: The evaluator may choose to include additional information that. Depending on the type of. Web tailor your evaluation to the patient’s conditions determine if a power mobility device is a necessary part of their treatment plan document that a mobility exam was a major. Web this form is for assessment of wheelchair users who cannot sit upright comfortably without support. How to fill out power wheelchair assessment form?. Utah medicaid prior authorization modification request form. Your physical abilities the accessibility of your environment your functional limitations your ability to perform mobility related activities of daily living. Web the therapist will evaluate: Jessica presperin pedersen, jill sparacio, mike babinec, julie piriano (2003,2007, 2014, 2018) 6/15.
Web the therapist will evaluate: Easily fill out pdf blank, edit, and sign them. Web wheelchair/scooter/stroller seating assessment form (ccp/home health services) (8 pages) f00098 page 2 of 8. Web this form must be completed by the licensed therapist or the certified physiatrist performing the evaluation. Is the pain such that it would prohibit the member from using a manual. Web complete medicare wheelchair evaluation template online with us legal forms. Depending on the type of. Keep this form in the wheelchair user’s file. Web urine drug screen information form. Web wheelchair and seating evaluation:
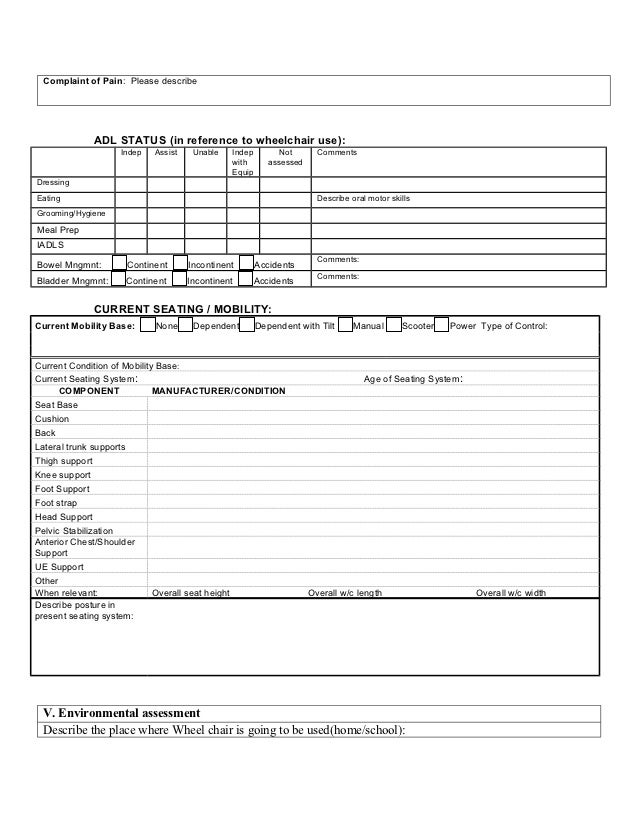
We must identify the primary as well as all potentially relevant secondary diagnoses: Save or instantly send your ready documents. Web wheelchair initial evaluation form april 2020 page 4 of 6 if yes, describe pain and level of intensity. Which of these is the reason for the need for wheeled mobility? Web the therapist will evaluate: Utah medicaid prior authorization modification request form. Web up to $40 cash back the assessment form is used to determine if a power wheelchair is the best mobility solution for the individual. Depending on the type of. Web complete medicare wheelchair evaluation template online with us legal forms. Web this form must be completed by the licensed therapist or the certified physiatrist performing the evaluation.
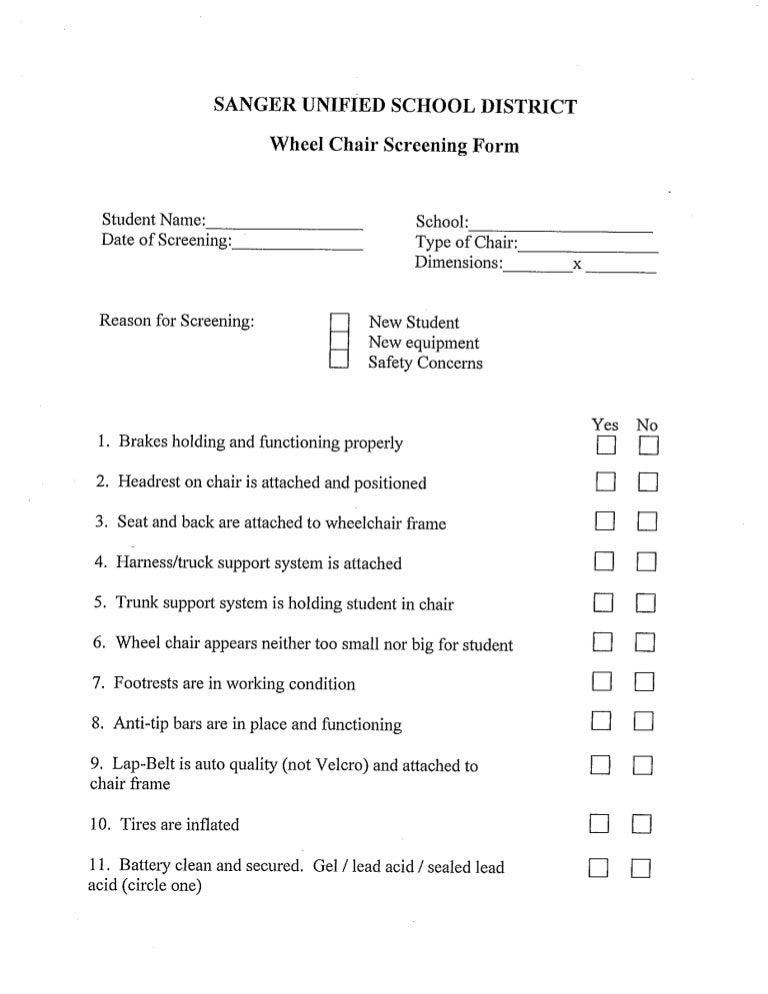
Wheel chair screening form
Jessica presperin pedersen, jill sparacio, mike babinec, julie piriano (2003,2007, 2014, 2018) 6/15. Web wheelchair and seating evaluation: How to fill out power wheelchair assessment form?. Web rx to evaluate and treat by physical medicine and rehabilitation for wheelchair/seating rx to evaluate and treat by physical or occupational therapy for wheelchair/seating. Your physical abilities the accessibility of your environment your.

Wheel chair assessment Form
Web wheelchair/scooter/stroller seating assessment form (ccp/home health services) (8 pages) f00098 page 2 of 8. Web urine drug screen information form. Jessica presperin pedersen, jill sparacio, mike babinec, julie piriano (2003,2007, 2014, 2018) 6/15. Web wheelchair and seating evaluation: Web medicare power wheelchair evaluation and documentation.
Medicare Manual Wheelchair Evaluation Form Form Resume Examples
Medicare pays for different kinds of dme in different ways. Web rx to evaluate and treat by physical medicine and rehabilitation for wheelchair/seating rx to evaluate and treat by physical or occupational therapy for wheelchair/seating. The evaluator may choose to include additional information that. Easily fill out pdf blank, edit, and sign them. How to fill out power wheelchair assessment.
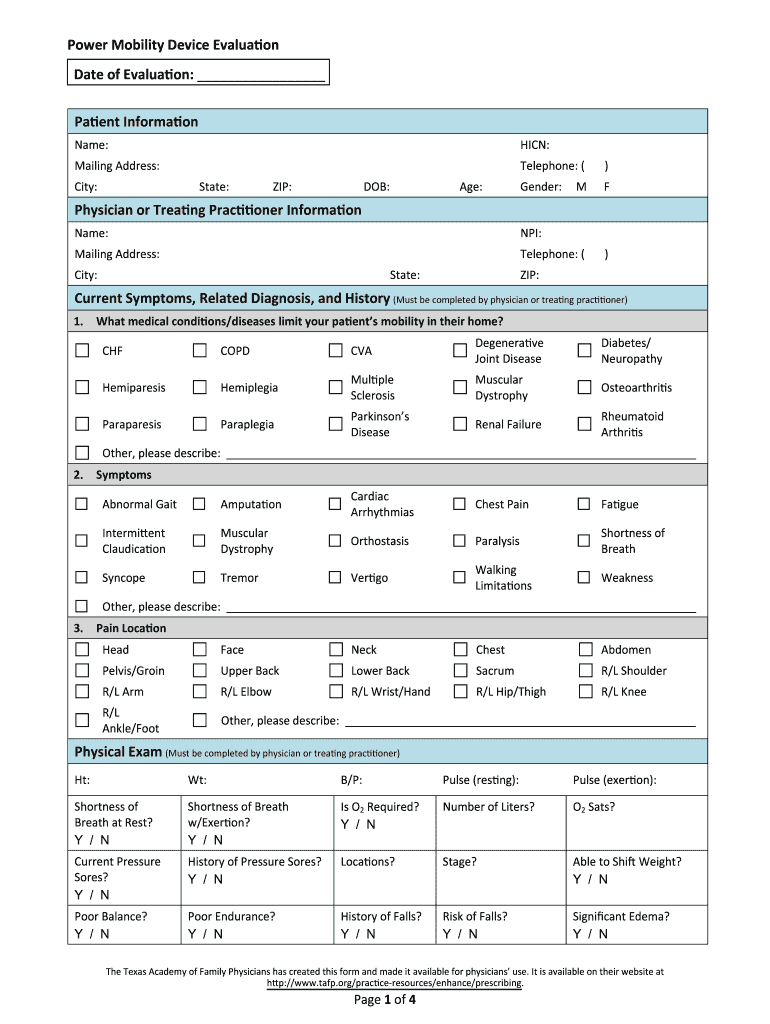
Power Mobility Device Evaluation Form Fill Out and Sign Printable PDF
We must identify the primary as well as all potentially relevant secondary diagnoses: How to fill out power wheelchair assessment form?. Web wheelchair initial evaluation form april 2020 page 4 of 6 if yes, describe pain and level of intensity. Easily fill out pdf blank, edit, and sign them. Depending on the type of.
Ohio Medicaid Wheelchair Evaluation Form Form Resume Examples
Web medicare power wheelchair evaluation and documentation. Medicare pays for different kinds of dme in different ways. Is the pain such that it would prohibit the member from using a manual. Your physical abilities the accessibility of your environment your functional limitations your ability to perform mobility related activities of daily living. Web wheelchair initial evaluation form april 2020 page.

Medicare Electric Wheelchair Form Form Resume Examples Dp3OEEr10Q
Web rx to evaluate and treat by physical medicine and rehabilitation for wheelchair/seating rx to evaluate and treat by physical or occupational therapy for wheelchair/seating. Which of these is the reason for the need for wheeled mobility? Web the therapist will evaluate: Web wheelchair initial evaluation form april 2020 page 4 of 6 if yes, describe pain and level of.
Wheel chair assessment Form
Depending on the type of. Web medicare power wheelchair evaluation and documentation. Web wheelchair initial evaluation form april 2020 page 4 of 6 if yes, describe pain and level of intensity. Web this form must be completed by the licensed therapist or the certified physiatrist performing the evaluation. Medicare pays for different kinds of dme in different ways.
Wheel chair assessment Form
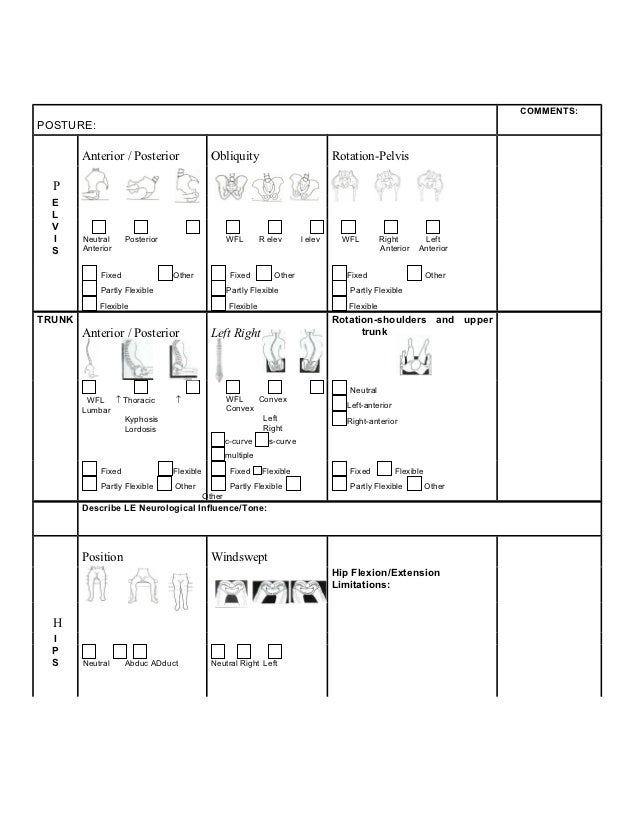
Jessica presperin pedersen, jill sparacio, mike babinec, julie piriano (2003,2007, 2014, 2018) 6/15. Web complete medicare wheelchair evaluation template online with us legal forms. Web this form is for assessment of wheelchair users who cannot sit upright comfortably without support. Which of these is the reason for the need for wheeled mobility? We must identify the primary as well as.
Wheel chair assessment Form
Utah medicaid prior authorization modification request form. Web this form must be completed by the licensed therapist or the certified physiatrist performing the evaluation. Depending on the type of. Web this form is for assessment of wheelchair users who cannot sit upright comfortably without support. Web tailor your evaluation to the patient’s conditions determine if a power mobility device is.

Wheelchair Assessment Fill Online, Printable, Fillable, Blank pdfFiller
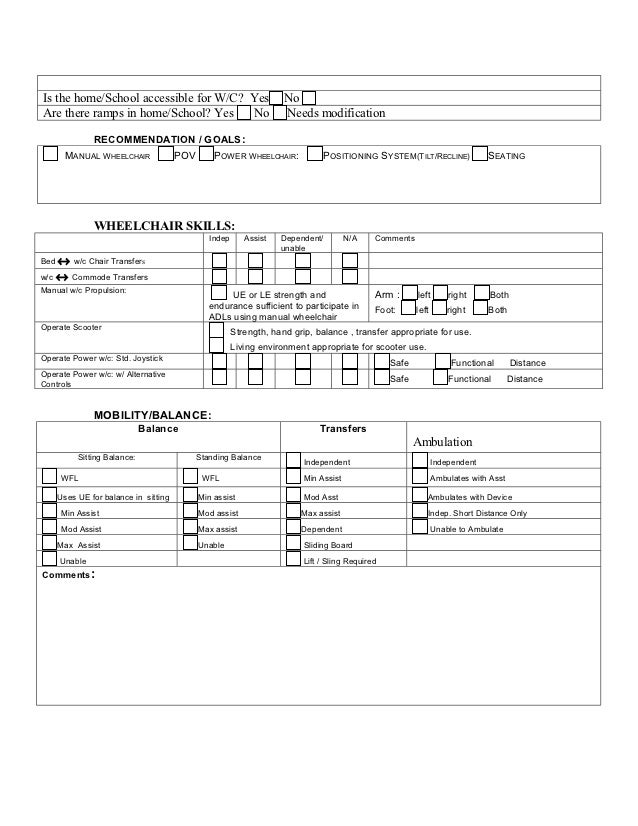
Your physical abilities the accessibility of your environment your functional limitations your ability to perform mobility related activities of daily living. Easily fill out pdf blank, edit, and sign them. Keep this form in the wheelchair user’s file. Web wheelchair initial evaluation form april 2020 page 4 of 6 if yes, describe pain and level of intensity. Which of these.
Web Medicare Power Wheelchair Evaluation And Documentation.
Web tailor your evaluation to the patient’s conditions determine if a power mobility device is a necessary part of their treatment plan document that a mobility exam was a major. Web wheelchair and seating evaluation: Web complete medicare wheelchair evaluation template online with us legal forms. Save or instantly send your ready documents.
Jessica Presperin Pedersen, Jill Sparacio, Mike Babinec, Julie Piriano (2003,2007, 2014, 2018) 6/15.
We must identify the primary as well as all potentially relevant secondary diagnoses: Your physical abilities the accessibility of your environment your functional limitations your ability to perform mobility related activities of daily living. Easily fill out pdf blank, edit, and sign them. Web urine drug screen information form.
Is The Pain Such That It Would Prohibit The Member From Using A Manual.
Which of these is the reason for the need for wheeled mobility? How to fill out power wheelchair assessment form?. Web the therapist will evaluate: Web this form must be completed by the licensed therapist or the certified physiatrist performing the evaluation.
Medicare Pays For Different Kinds Of Dme In Different Ways.
Depending on the type of. Web wheelchair/scooter/stroller seating assessment form (ccp/home health services) (8 pages) f00098 page 2 of 8. Web this form is for assessment of wheelchair users who cannot sit upright comfortably without support. Keep this form in the wheelchair user’s file.