Xolair Consent Form
Xolair Consent Form - Web two forms are needed to enroll in the genentech patient foundation: Prescriber foundation form (to be completed by the health care provider). For patients prescribed prxolair® for moderate to severe allergic asthma (aa) or chronic idiopathic urticaria (ciu) all sections must be completely filled out (please print) phone: *programs have specific eligibility criteria. Patient consent form (to be completed by the patient). Web xolair therapy patient consent i, ______________________________ am acknowledging that i will begin my xolair treatment. Welcome to omic's license form library, a collection of loss proactive or patient education create on ophthalmic practices. Web xolair is a medication for patients 12 years of age or older with moderate to severe persistent allergic asthma whose asthma symptoms are not well controlled by asthma medicines. The nature and purpose of xolair treatment program Fda approval letter (follow here connection and search the and drug name) prescribing information.
Fda approval letter (follow here connection and search the and drug name) prescribing information. For more information, visit genentechpatientfoundation.com. Web use the links below to find additional information to encompass in your letter. Web two forms are needed to enroll in the genentech patient foundation: Prescriber foundation form (to be completed by the health care provider). The nature and purpose of xolair treatment program Web xolair is a medication for patients 12 years of age or older with moderate to severe persistent allergic asthma whose asthma symptoms are not well controlled by asthma medicines. Web start enrollment with the patient consent form to get started, fill out the patient consent form. You can submit this form in 1 of 3 ways: Welcome to omic's license form library, a collection of loss proactive or patient education create on ophthalmic practices.
(print name legibly) the following points regarding xolair were reviewed and discussed in great detail: Prescriber foundation form (to be completed by the health care provider). Web use the links below to find additional information to encompass in your letter. For patients prescribed prxolair® for moderate to severe allergic asthma (aa) or chronic idiopathic urticaria (ciu) all sections must be completely filled out (please print) phone: Web two forms are needed to enroll in the genentech patient foundation: The nature and purpose of xolair treatment program You can submit this form in 1 of 3 ways: Web start enrollment with the patient consent form to get started, fill out the patient consent form. Fda approval letter (follow here connection and search the and drug name) prescribing information. Web xolair is a medication for patients 12 years of age or older with moderate to severe persistent allergic asthma whose asthma symptoms are not well controlled by asthma medicines.
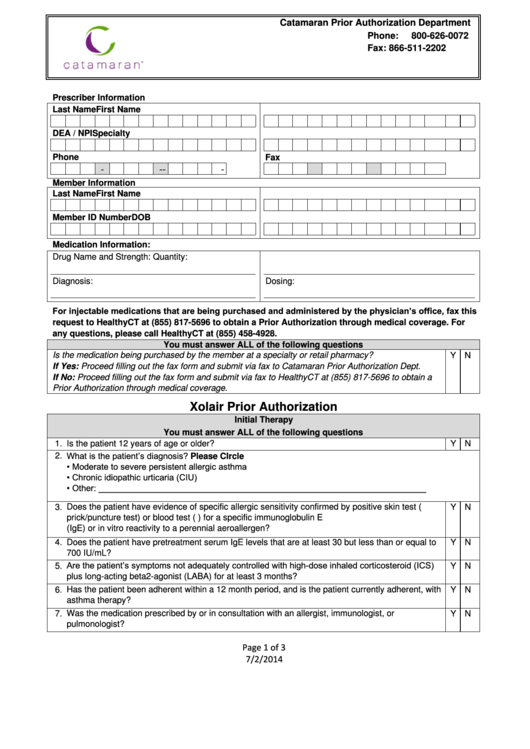
Xolair Prior Authorization Healthyct printable pdf download
For patients prescribed prxolair® for moderate to severe allergic asthma (aa) or chronic idiopathic urticaria (ciu) all sections must be completely filled out (please print) phone: The nature and purpose of xolair treatment program Web xolair therapy patient consent i, ______________________________ am acknowledging that i will begin my xolair treatment. Web use the links below to find additional information to.

Xhale+ Xolair Enrolment Consent Form Juno EMR Support Portal
Web two forms are needed to enroll in the genentech patient foundation: Web xhale+ program patient enrolment and consent form: You can submit this form in 1 of 3 ways: Fda approval letter (follow here connection and search the and drug name) prescribing information. Unless encrypted, be mindful that email communications may not be safe.

ALL ALLERGY AND ASTHMA CARE XOLAIR TREATMENT FOR HIVES
Welcome to omic's license form library, a collection of loss proactive or patient education create on ophthalmic practices. (print name legibly) the following points regarding xolair were reviewed and discussed in great detail: Prescriber foundation form (to be completed by the health care provider). Web xolair therapy patient consent i, ______________________________ am acknowledging that i will begin my xolair treatment..

How to Pronounce Xolair YouTube
Fda approval letter (follow here connection and search the and drug name) prescribing information. Web start enrollment with the patient consent form to get started, fill out the patient consent form. Web xolair is a medication for patients 12 years of age or older with moderate to severe persistent allergic asthma whose asthma symptoms are not well controlled by asthma.

Xolair Patient Consent Form 2023
Web two forms are needed to enroll in the genentech patient foundation: Welcome to omic's license form library, a collection of loss proactive or patient education create on ophthalmic practices. Web start enrollment with the patient consent form to get started, fill out the patient consent form. Web xhale+ program patient enrolment and consent form: Web patient enrollment and consent.

XOLAIR Dosage & Rx Info Uses, Side Effects The Clinical Advisor
Web xolair is a medication for patients 12 years of age or older with moderate to severe persistent allergic asthma whose asthma symptoms are not well controlled by asthma medicines. Web start enrollment with the patient consent form to get started, fill out the patient consent form. *programs have specific eligibility criteria. Unless encrypted, be mindful that email communications may.

Alternatives To Xolair For Hives kalcicdesignandphotography
Web start enrollment with the patient consent form to get started, fill out the patient consent form. Patient consent form (to be completed by the patient). Web xhale+ program patient enrolment and consent form: Prescriber foundation form (to be completed by the health care provider). For patients prescribed prxolair® for moderate to severe allergic asthma (aa) or chronic idiopathic urticaria.
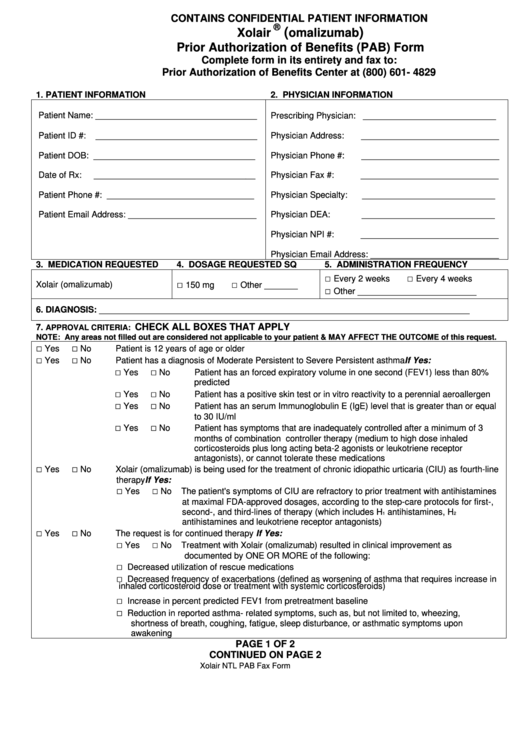
Xolair (Omalizumab) Prior Authorization Of Benefits (Pab) Form
Web xolair is a medication for patients 12 years of age or older with moderate to severe persistent allergic asthma whose asthma symptoms are not well controlled by asthma medicines. You can submit this form in 1 of 3 ways: Web patient enrollment and consent form for patients prescribed prxolair® for chronic idiopathic urticaria (ciu), all sections must be completely.

Xolair Indications/Uses MIMS Hong Kong
Web xolair is a medication for patients 12 years of age or older with moderate to severe persistent allergic asthma whose asthma symptoms are not well controlled by asthma medicines. You can submit this form in 1 of 3 ways: See full prescribing, safe, & boxed warning info. The nature and purpose of xolair treatment program Web xolair therapy patient.
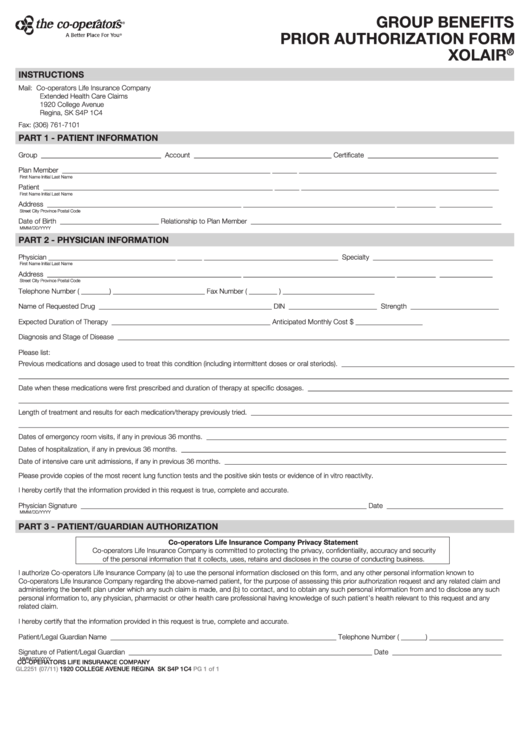
Fillable Form Gl2251 Group Benefits Prior Authorization Xolair
Web xolair is a medication for patients 12 years of age or older with moderate to severe persistent allergic asthma whose asthma symptoms are not well controlled by asthma medicines. Web use the links below to find additional information to encompass in your letter. Web xolair therapy patient consent i, ______________________________ am acknowledging that i will begin my xolair treatment..
For More Information, Visit Genentechpatientfoundation.com.
(print name legibly) the following points regarding xolair were reviewed and discussed in great detail: *programs have specific eligibility criteria. See full prescribing, safe, & boxed warning info. A skin or blood test is done to confirm you have allergic asthma.
Prescriber Foundation Form (To Be Completed By The Health Care Provider).
Patient consent form (to be completed by the patient). Welcome to omic's license form library, a collection of loss proactive or patient education create on ophthalmic practices. Web patient enrollment and consent form for patients prescribed prxolair® for chronic idiopathic urticaria (ciu), all sections must be completely filled out (please print). Web if you think your patient qualifies for xolair access solutions, submit the completed prescriber service form and respiratory patient consent form to genentech access solutions.
The Nature And Purpose Of Xolair Treatment Program
Fda approval letter (follow here connection and search the and drug name) prescribing information. Web xhale+ program patient enrolment and consent form: Unless encrypted, be mindful that email communications may not be safe. Web start enrollment with the patient consent form to get started, fill out the patient consent form.
Web Use The Links Below To Find Additional Information To Encompass In Your Letter.
You can submit this form in 1 of 3 ways: For patients prescribed prxolair® for moderate to severe allergic asthma (aa) or chronic idiopathic urticaria (ciu) all sections must be completely filled out (please print) phone: Web xolair therapy patient consent i, ______________________________ am acknowledging that i will begin my xolair treatment. Web xolair is a medication for patients 12 years of age or older with moderate to severe persistent allergic asthma whose asthma symptoms are not well controlled by asthma medicines.