Ada Dental Claim Form 2022 Pdf
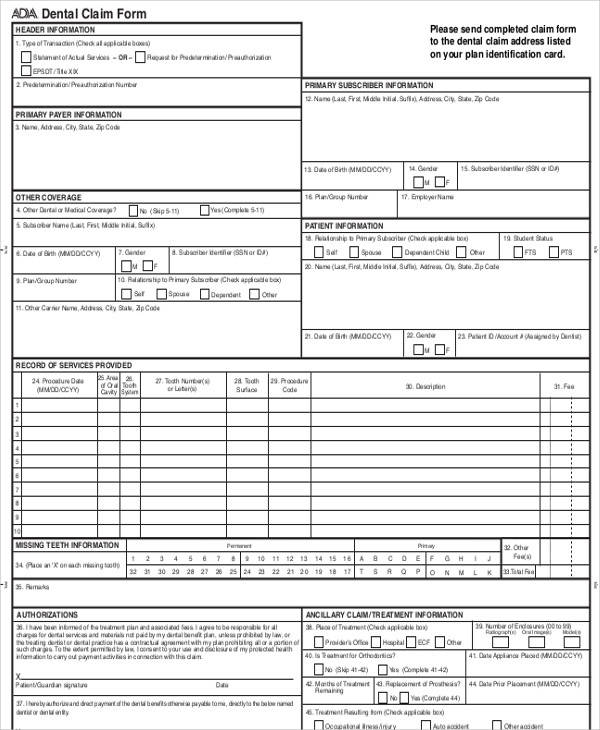
Ada Dental Claim Form 2022 Pdf - Web insurance company/dental benefit plan information 3. Edit your ada dental claim form printable online. This information is required when the diagnosis may affect claim adjudication when specific. This information is required when the diagnosis may affect claim adjudication when specific. Access ada dental claim form now at no cost! Ad 2006 ada j400 & more fillable forms, register and subscribe now! Save or instantly send your ready documents. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental. Web the form supports reporting up to four diagnosis codes per dental procedure. Web dental claim form type of transaction (mark all applicable boxes) statement of actual servicesrequest for predetermination/preauthorization epsdt / title xix.
Web comprehensive ada dental claim form completion instructions are printed in the cdt manual. Date of birth (mm/dd/ccyy) 14. This information is required when the diagnosis may affect claim adjudication when specific. This information is required when the diagnosis may affect claim adjudication when specific. Any updates to these instructions will be posted on the ada’s web site. Edit your ada dental claim form printable online. Web the form supports reporting up to four diagnosis codes per dental procedure. Easily fill out pdf blank, edit, and sign them. Patient’s name (first, middle initial, last) 4. Web insurance company/dental benefit plan information 3.
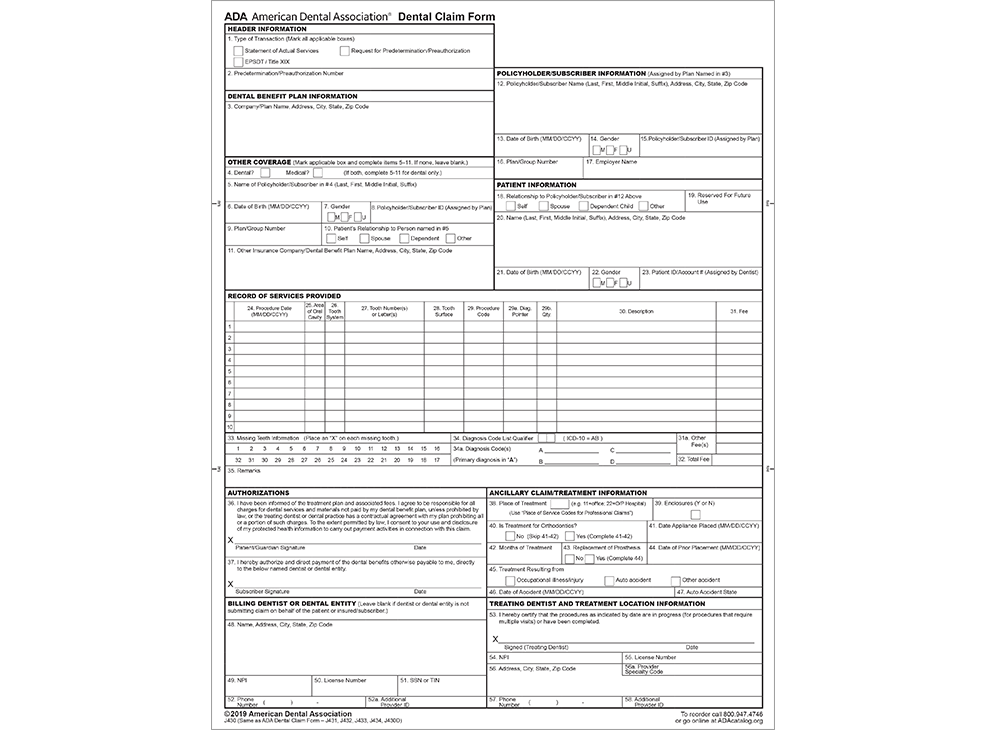
Web the form supports reporting up to four diagnosis codes per dental procedure. Web ada dental claim form sample unless the following sections of a dental bill are completed correctly, the bill will be returned and payment may be delayed. This information is required when the diagnosis may affect claim adjudication when specific. This information is required when the diagnosis may affect claim adjudication when specific. Web insurance company/dental benefit plan information 3. Date of birth (mm/dd/ccyy) 14. Web ada dental claim form completion instructions version 2019 © american dental association page 1 of 16. Access ada dental claim form now at no cost! Easily fill out pdf blank, edit, and sign them. Sign it in a few clicks.

ADA Dental Form
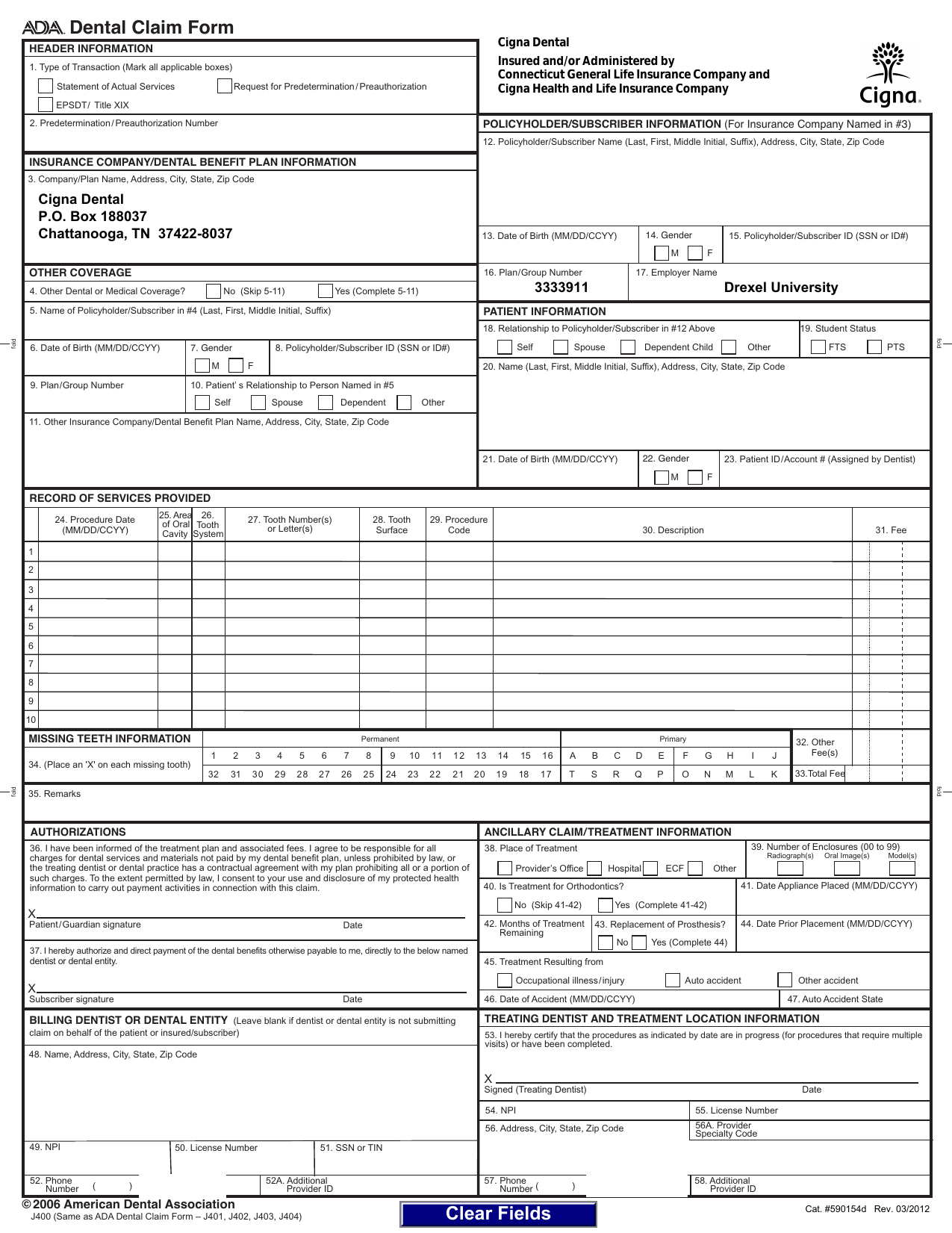
Version 2024 © american dental association. Web looking for ada dental claim form? Web dental claim form type of transaction (mark all applicable boxes) statement of actual servicesrequest for predetermination/preauthorization epsdt / title xix. Edit your ada dental claim form printable online. This information is required when the diagnosis may affect claim adjudication when specific.
Printable Ada Claim Form 2021 Printable World Holiday
Five relevant extracts from that. Web dental claim form type of transaction (mark all applicable boxes) statement of actual servicesrequest for predetermination/preauthorization epsdt / title xix. Web dental claim form please type or print 1. Web insurance company/dental benefit plan information 3. Group number or enrollment code 3.
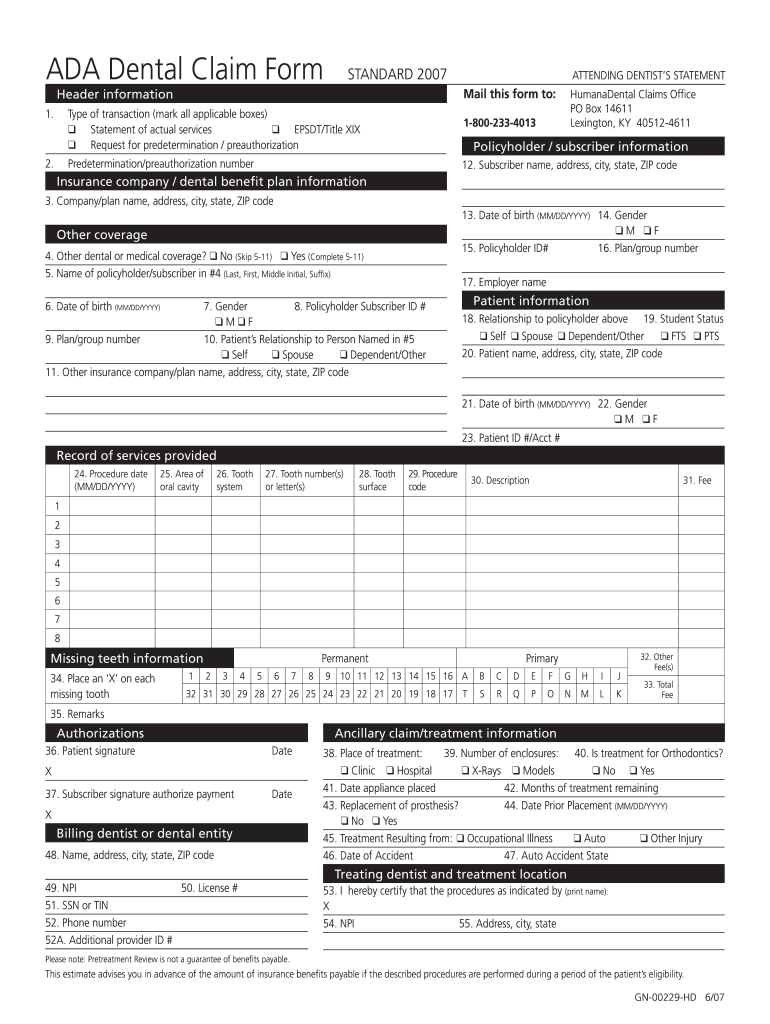
Humana Dental Claim Form 20072022 Fill Out and Sign Printable PDF
Edit your ada dental claim form printable online. Date of birth (mm/dd/ccyy) 14. Patient’s name (first, middle initial, last) 4. Company/plan name, address, city, state, zip code submit claim forms to: Web dental claim form please type or print 1.

ADA Dental Claim Form Changes Dental Medical Billing
Group number or enrollment code 3. Web insurance company/dental benefit plan information 3. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental. Date of birth (mm/dd/ccyy) 14. Version 2024 © american dental association.

Medical Office Supplies
Save or instantly send your ready documents. Group number or enrollment code 3. This information is required when the diagnosis may affect claim adjudication when specific. This information is required when the diagnosis may affect claim adjudication when specific. Sign it in a few clicks.
Dental Claim Form, downloadable PDF ADA J430D
Web ada dental claim form completion instructions. Web ada dental claim form sample unless the following sections of a dental bill are completed correctly, the bill will be returned and payment may be delayed. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and.
Dental Claim Form
Web the form supports reporting up to four diagnosis codes per dental procedure. Web the form supports reporting up to four diagnosis codes per dental procedure. Patient’s name (first, middle initial, last) 4. Access ada dental claim form now at no cost! Web insurance company/dental benefit plan information 3.

WADA2019CS 2019 NEW ADA Dental Claim Form StockChecks
This information is required when the diagnosis may affect claim adjudication when specific. Web ada dental claim form completion instructions version 2019 © american dental association page 1 of 16. Web the form supports reporting up to four diagnosis codes per dental procedure. Web ada dental claim form sample unless the following sections of a dental bill are completed correctly,.
Printable Ada Claim Form 2021 Printable World Holiday
Web comprehensive ada dental claim form completion instructions are printed in the cdt manual. Sign it in a few clicks. Date of birth (mm/dd/ccyy) 14. Company/plan name, address, city, state, zip code submit claim forms to: Web dental claim form type of transaction (mark all applicable boxes) statement of actual servicesrequest for predetermination/preauthorization epsdt / title xix.
Vitality Dental Claim Form designunie
Patient’s name (first, middle initial, last) 4. Group number or enrollment code 3. This information is required when the diagnosis may affect claim adjudication when specific. On formspal, you can get this form and change or complete it with our pdf tool online. Web the form supports reporting up to four diagnosis codes per dental procedure.
Easily Fill Out Pdf Blank, Edit, And Sign Them.
Any updates to these instructions will be posted on the ada’s web site. Version 2024 © american dental association. Access ada dental claim form now at no cost! Web ada dental claim form sample unless the following sections of a dental bill are completed correctly, the bill will be returned and payment may be delayed.
Patient’s Name (First, Middle Initial, Last) 4.
Date of birth (mm/dd/ccyy) 14. Web dental claim form header information type of transaction (mark all applicable boxes) statement of actual services request for predetermination/preauthorization. Web looking for ada dental claim form? Sign it in a few clicks.
Company/Plan Name, Address, City, State, Zip Code Submit Claim Forms To:
Save or instantly send your ready documents. This information is required when the diagnosis may affect claim adjudication when specific. Web the form supports reporting up to four diagnosis codes per dental procedure. This information is required when the diagnosis may affect claim adjudication when specific.
Web Ada Dental Claim Form Completion Instructions.
Group number or enrollment code 3. Ad 2006 ada j400 & more fillable forms, register and subscribe now! Five relevant extracts from that. On formspal, you can get this form and change or complete it with our pdf tool online.