Ub 04 Form Aflac
Ub 04 Form Aflac - Sign it in a few clicks. Edit your ub 04 form pdf fillable online. This would include things like surgery, radiology, laboratory, or other. Web form locator required field field name comments if the frequency code indicates an adjustment of a prior claim (7, 8), the original claim id (as assigned by thp), must be. Then you can do either of the following: 1 required enter the billing provider’s name, street address, city, state, and zip code. The centers for medicare and medicaid (cms). Upload, modify or create forms. Web the ub04 claim form is used to submit claims for inpatient and outpatient services by institutional facilities (for example, outpatient departments, rural health clinics, chronic. Type text, add images, blackout confidential details, add comments, highlights and more.
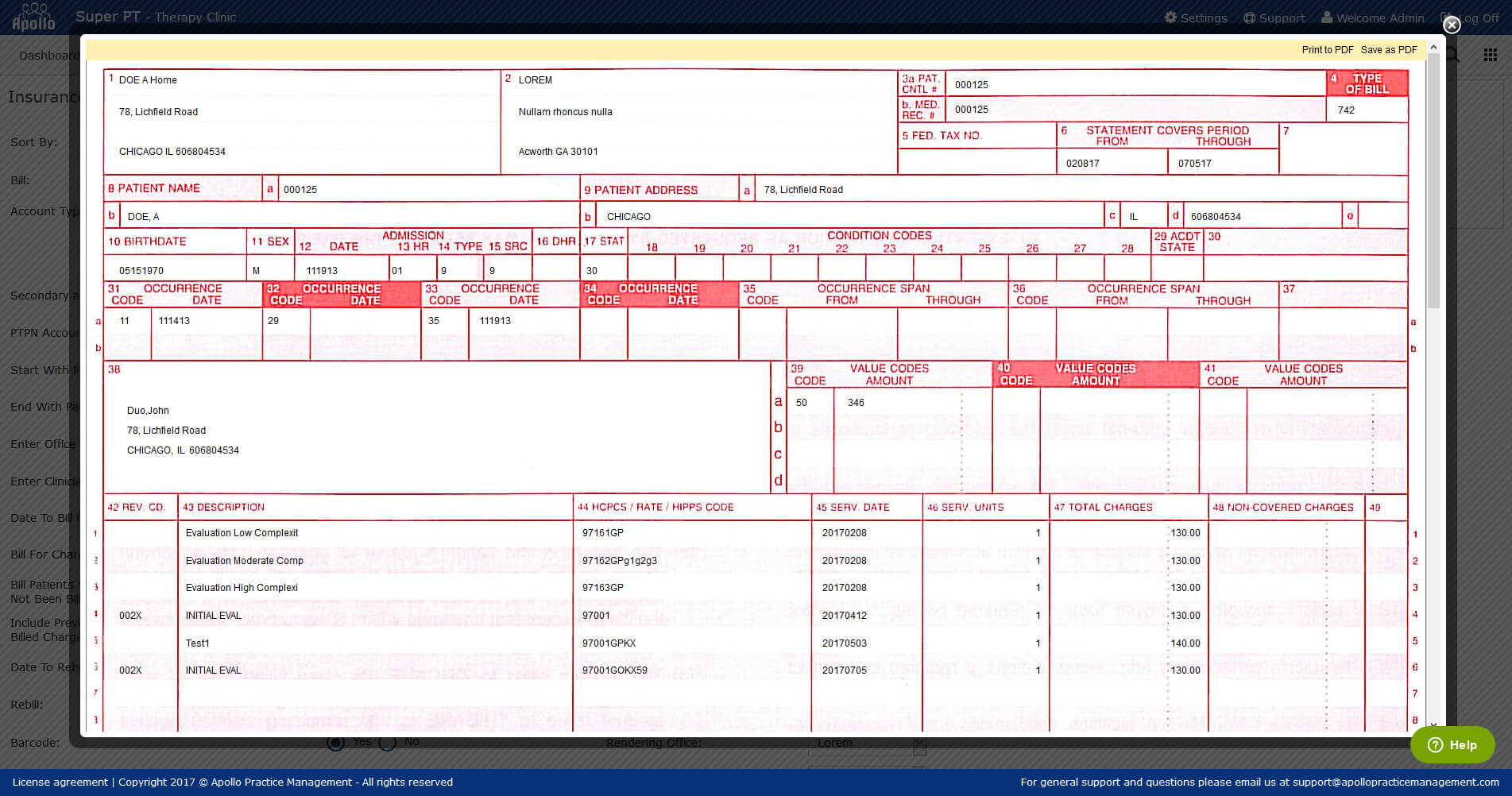
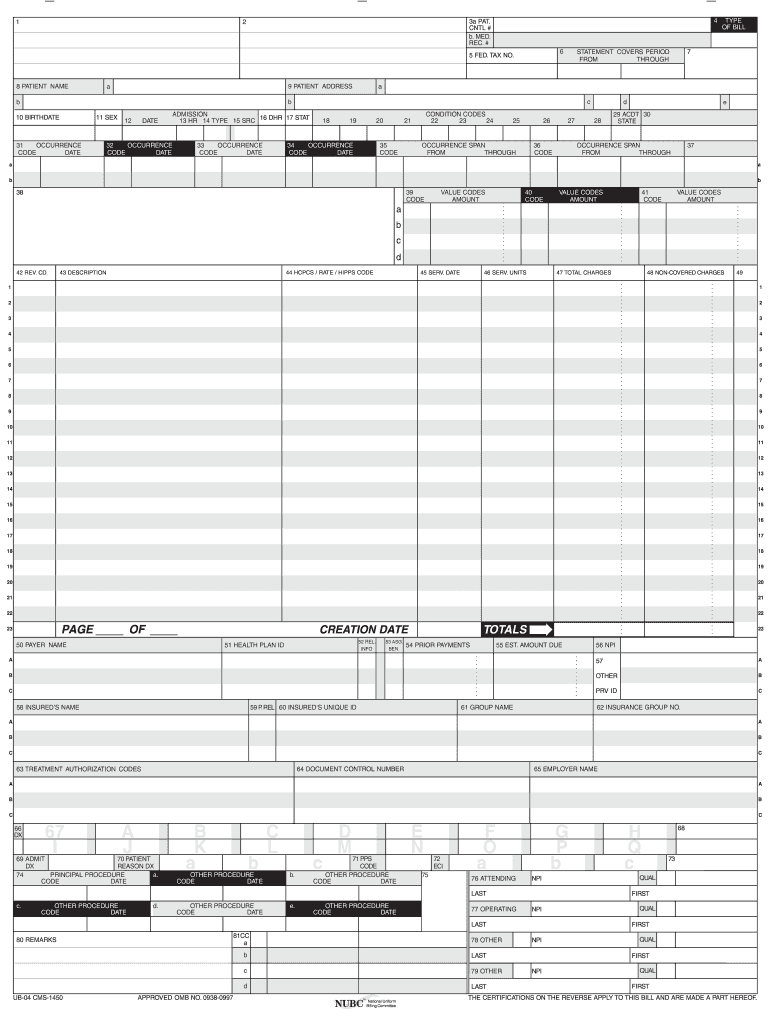
Web the ub04 claim form is used to submit claims for inpatient and outpatient services by institutional facilities (for example, outpatient departments, rural health clinics, chronic. Upload, modify or create forms. Type text, add images, blackout confidential details, add comments, highlights and more. Web form locator required field field name comments if the frequency code indicates an adjustment of a prior claim (7, 8), the original claim id (as assigned by thp), must be. The centers for medicare and medicaid (cms). This would include things like surgery, radiology, laboratory, or other. 1 required enter the billing provider’s name, street address, city, state, and zip code. Try it for free now! For this version of the forms, once you fill in the form, click the “i’m finished!” button at the very bottom of the form. Sign it in a few clicks.
1 required enter the billing provider’s name, street address, city, state, and zip code. Web form locator required field field name comments if the frequency code indicates an adjustment of a prior claim (7, 8), the original claim id (as assigned by thp), must be. Ad download or email form ub04 & more fillable forms, register and subscribe now! Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to you. Edit your ub 04 form pdf fillable online. Web the ub04 claim form is used to submit claims for inpatient and outpatient services by institutional facilities (for example, outpatient departments, rural health clinics, chronic. Sign it in a few clicks. Type text, add images, blackout confidential details, add comments, highlights and more. Try it for free now! The centers for medicare and medicaid (cms).
Physical Therapy Billing Software PT Billing Software Apollo
This would include things like surgery, radiology, laboratory, or other. The centers for medicare and medicaid (cms). Upload, modify or create forms. Sign it in a few clicks. Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to you.

6 Ub 04 form Template FabTemplatez
This would include things like surgery, radiology, laboratory, or other. For this version of the forms, once you fill in the form, click the “i’m finished!” button at the very bottom of the form. Edit your ub 04 form pdf fillable online. Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at.

Gallery of Ub 04 form Aflac Unique Health Insurance Claim form form
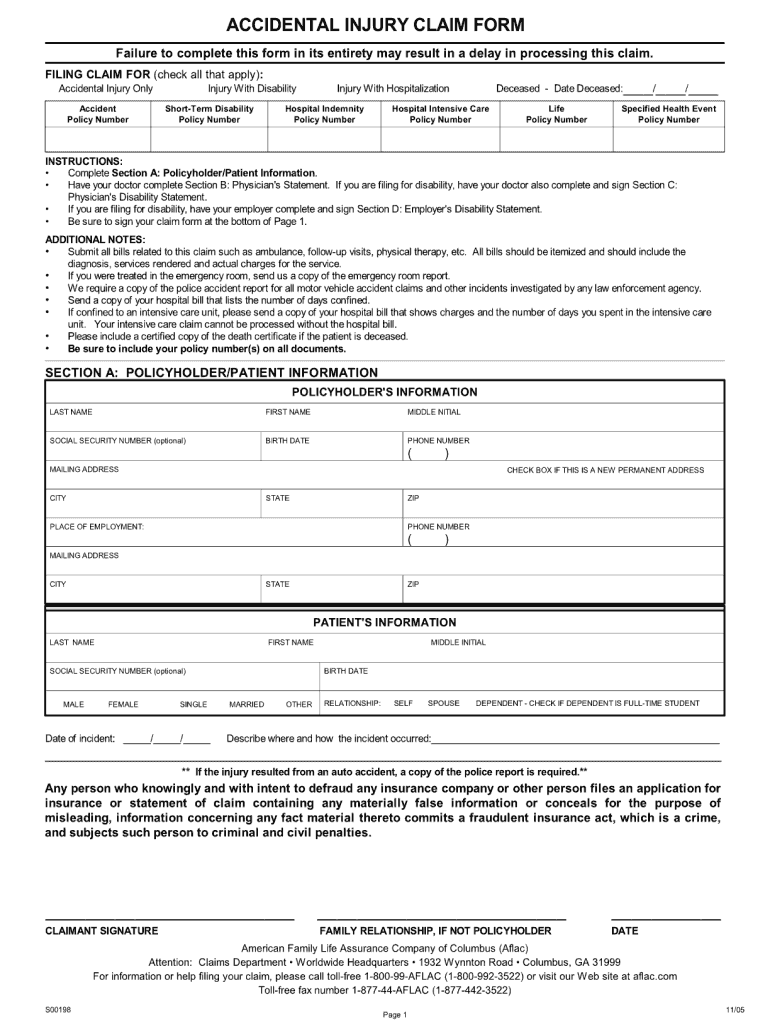
Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to you. This would include things like surgery, radiology, laboratory, or other. Try it for free now! Ad download or email form ub04 & more fillable forms, register and subscribe now! 1 required enter the.

Printable Ub 04 Claim Form Printable Forms Free Online
Try it for free now! Web the ub04 claim form is used to submit claims for inpatient and outpatient services by institutional facilities (for example, outpatient departments, rural health clinics, chronic. For this version of the forms, once you fill in the form, click the “i’m finished!” button at the very bottom of the form. Upload, modify or create forms..
Ub04 claim forms Fill out & sign online DocHub
The centers for medicare and medicaid (cms). Then you can do either of the following: Ad download or email form ub04 & more fillable forms, register and subscribe now! For this version of the forms, once you fill in the form, click the “i’m finished!” button at the very bottom of the form. Web the ub04 claim form is used.
Aflac Printable Claim Forms
Sign it in a few clicks. For this version of the forms, once you fill in the form, click the “i’m finished!” button at the very bottom of the form. Edit your ub 04 form pdf fillable online. Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the.

Gallery of Ub 04 form Aflac Unique Health Insurance Claim form form
Ad download or email form ub04 & more fillable forms, register and subscribe now! This would include things like surgery, radiology, laboratory, or other. Type text, add images, blackout confidential details, add comments, highlights and more. Try it for free now! For this version of the forms, once you fill in the form, click the “i’m finished!” button at the.

Gallery of Ub 04 form Aflac Unique Ub 04 form Sample Luxury 1500 Claim
For this version of the forms, once you fill in the form, click the “i’m finished!” button at the very bottom of the form. Upload, modify or create forms. The centers for medicare and medicaid (cms). Edit your ub 04 form pdf fillable online. Type text, add images, blackout confidential details, add comments, highlights and more.

Gallery of Ub 04 form Aflac Unique Health Insurance Claim form form
Try it for free now! For this version of the forms, once you fill in the form, click the “i’m finished!” button at the very bottom of the form. Edit your ub 04 form pdf fillable online. Web form locator required field field name comments if the frequency code indicates an adjustment of a prior claim (7, 8), the original.
Recording Additional Information on the UB04 Form
Upload, modify or create forms. Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to you. Edit your ub 04 form pdf fillable online. The centers for medicare and medicaid (cms). Web the ub04 claim form is used to submit claims for inpatient and.
Then You Can Do Either Of The Following:
Ad download or email form ub04 & more fillable forms, register and subscribe now! Sign it in a few clicks. Try it for free now! Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to you.
Web Form Locator Required Field Field Name Comments If The Frequency Code Indicates An Adjustment Of A Prior Claim (7, 8), The Original Claim Id (As Assigned By Thp), Must Be.
Web the ub04 claim form is used to submit claims for inpatient and outpatient services by institutional facilities (for example, outpatient departments, rural health clinics, chronic. This would include things like surgery, radiology, laboratory, or other. Edit your ub 04 form pdf fillable online. Type text, add images, blackout confidential details, add comments, highlights and more.
The Centers For Medicare And Medicaid (Cms).
1 required enter the billing provider’s name, street address, city, state, and zip code. For this version of the forms, once you fill in the form, click the “i’m finished!” button at the very bottom of the form. Upload, modify or create forms.